Download
1 / 16
460 likes | 1.92k Views
ANTIFUNGAL DRUGS . Fungal infections (mycoses) can be both superficial and systemic. Superficial infections (Oral and vulvovaginal candidiasis, Dermatophytosis, e.g. Tinea pedis, Tinea corporis, ringworm, etc.)

E N D
ANTIFUNGAL DRUGS Fungal infections (mycoses) can be both superficial and systemic. Superficial infections (Oral and vulvovaginal candidiasis, Dermatophytosis, e.g. Tinea pedis, Tinea corporis, ringworm, etc.) Systemic infections (Candidiasis, Cryptococcal meningitis, Aspergillosis, Blastomycosis). Pulmonary aspergillosis is a leading cause of death in immunecompromised patients.
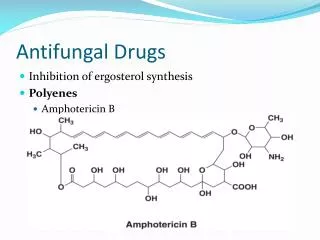
Polyene Antibiotics (Amphotericin-B and Nystatin) Mechanism: Fungal cell membranes, unlike mammalian cells and bacteria, contain large amount of ergosterol. Polyene antibiotics bind to plasma membrane ergosterol, damage membrane, and cause leakage of potassium ions.
Amphotericin B Broad spectrum antifungal effective against most systemic fungal infections. Not absorbed orally; parenteral only. Relatively high toxicity – nephrotoxic, neurotoxic at high dose Nystatin Similar to Amphotericin B. Not absorbed orally; topical only. Higher toxicity than A.B. – not given systemically Used to treat oral and esophageal Candidiasis (Thrush)
Azoles---Synthetic fungicidal agents Mechanism Azoles inhibit ergosterol synthesis by blocking Ianosine 14a-demethylase, a fungal CYP which converts lanosterol to ergosterol. This leads to increase membrane fluidity and permeability and inhibition of fungal cell growth and replication. Generally well absorbed and non toxic. Most generally useful drugs for superficial fungal infections, also useful for systemic infections. Can be administered both topically and systemically Potential inhibition of human CYP, especially ketoconazole
Azole Antifungals Ketoconazole: First azole, used only topically now. Relatively narrower spectrum, higher toxicity. Inhibitor of CYP3A4. Requires high gastric acidity for efficient absorption. Available as non-Rx ointment. Fluconazole: Most commonly prescribed systemic antifungal. Well absorbed orally, well tolerated. Drug of choice for most Candidiasis infections. Enters CNS (fungal meningitis). Less effective vs. Aspergillis. Itraconazole: Requires low pH for absorption. Does not inhibit steroidogenesis. Useful systemically vs. onychomycosis, deep (cryptic) non-CNS mycoses. More toxic than Fluconazole. More effective vs. Aspergillis. Clotrimazole: Available non-Rx, used topically only, for vulvo-vaginal candidiasis (“yeast infection”), oral candidiasis (as lozenge), ointment for “athlete’s foot”, “jock rash”(Dermatophytosis)
Allylamine Antifungals(Terbinafine) Also inhibit Ergosterol biosynthesis, by blocking squalene epoxidase (lanosterol precursor)
Terbinafine Concentrated in keratin, used for dermatophytosis (ringworm). Given both topically and p.o. Well tolerated, does not inhibit CYP Has replaced Griseofulvin for tmt of onychomycosis
Griseofulvin Acts as a fungistatic agent by binding to microtubules, causing inhibition of mitosis. Induces human CYP and causes multiple drug interactions. Rarely used now, (Terbinafine preferred) but still prescribed. Not effective topically.
Flucytosine Mechanism: Flucytosine is converted to 5-fluorouracil (5-FU) in fungal cells by cytosine deaminase. 5-FU inhibits thymidylate synthetase and DNA synthesis. Humans lack cytosine deaminase. Fungistatic.
Flucytosine Synthetic fluorinated pyrimidine. Narrow spectrum fungistatic agent, well absorbed after oral administration. Its concentration in CSF is 50-90% that in plasma. Combination with Amphotericin B is highly effective for Cryptococcal meningitis. Less toxic than amphotericin-B.
Echinocandins Natural product antibiotics, block cell wall formation and maintenance
Caspofungin Useful vs. systemic mycoses, e.g. cryptic Aspergillis (invasive aspergillosis) and Candida (esophageal candidiasis), especially in azole resistance or amphotericin B intolerance. Not absorbed from GI tract; administered by iv infusion once daily
Candidiasis Treatment: Topical and Systemic Drugs • Topical antifungals for localized candidiasis in patients with normal immune function. Nystatin oral suspension Rinse with 1 teaspoonful (5 ml)for two minutes, use q.i.d. (after meals, and at bedtime) and spit out. (Patient can be directed to rinse and swallow if there is pharyngeal involvement). Clotrimazole troches, 10 mg Dissolve in mouth 5 times per day for 14 days. Do not chew. • Systemic antifungals for disseminated disease and/or in immunocompromised patients. Fluconazole tablets, 100 mg/day Itraconazole tablets, 200 mg/day