Download
1 / 63
• 630 likes • 849 Views
Adrenogenital syndrome : Congenital adrenal hyperplasia (CAH): Genetic lesions in steroidogenesis. Congenital adrenal hyperplasia Autosomal recessive defects Result in diminished synthesis of cortisol In response to adrenal insufficiency POMC – ACTH increase

E N D
Adrenogenitalsyndrome: Congenital adrenal hyperplasia (CAH):Geneticlesions in steroidogenesis
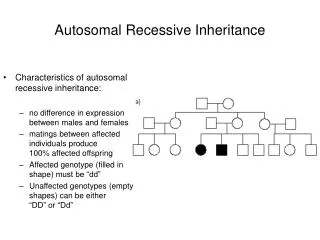
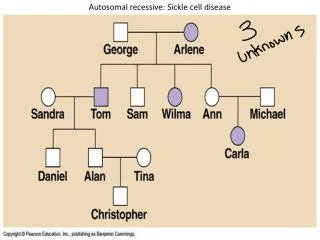
Congenital adrenal hyperplasia • Autosomal recessive defects • Result in diminished synthesis of cortisol • In response to adrenal insufficiency POMC – ACTH increase • ACTH + possibly other peptides derived from the amino-terminal end of POMC stimulate adrenal hypertrophy and hyperplasia (most prominent finding at autopsy).
Theory CAH is easy to understand: The signs and symptoms of the disease derive from the deficiency of the steroidal end product and the effects of accumulated steroidal precursors proximal to the blocked step.
Practice Because each steroidogenic enzyme has multiple activities and many extra-adrenal tissues contain enzymes that have similar activity, the complete elimination of a specific adrenal enzyme may not result in the complete elimination of its steroidal products from the circulation CAH can be confusing.
Example: • 3ß – HSD deficiency • Affected infants should have low 17 OHP. • Due to extraadrenal 3ß – HSD-I have very high 17-OHP.
Congenital lipoid adrenal hyperplasia: • Most severe genetic disorder of steroid hormone synthesis. • Absence of significant concentrations of all steroids • High basal ACTH and plasma renin activity
Congenital lipoid adrenal hyperplasia: • Cholesterol transport to the mitochondria is affected (steroidogenic regulatory protein: StAR). • Only disorder in steroid hormone biosynthesis that is not caused by a disrupted steroidogenic enzyme. • Salt-wasting crisis, 46XYDSD
3ß hydroxysteroid dehydrogenase deficiency Classic form: Genetic females have cliteromegaly + mild virilization because the fetal adrenal overproduces large amounts of DHEA, a small portion of which is converted to testosterone by extra-adrenal 3ß HSD Type 1 Genetic males: small phallus+ severe hypospadias
3ß hydroxysteroid dehydrogenase deficiency: Mild-partial defects: Young girls with premature adrenarche or young women with a history of premature adrenarche + complaints of hirsutism, virilism and oligomenorrhoea.
17 α hydroxylase – 17,20 lyase deficiency: P450c17 has both 17αhydroxylase and 17-20 lyase activities Deficient 17 α hydroxylase activity different clinical manifestations of Deficient 17-20 lyase activitydifferent lesions in the same gene
17 α hydroxylase – 17,20 lyase deficiency: • Overproduction of corticosterone (glucocorticoid activity) • Overproduction of DOC (sodium retention, hypertension and hypokalaemia, suppressed renin activity and aldosterone secretion)
17α hydroxylase – 17,20 lyase deficiency: Affected females: phenotypically normal but fail to undergo adrenarche and puberty. Affected males: absent or incomplete development of the external genitalia
17α hydroxylase – 17,20 lyase deficiency: Classic presentation: teenage girl with sexual infantilism and hypertension
21 hydroxylase deficiency: Due to mutations in the gene encoding adrenal P450c21 One of the most common inborn errors of metabolism and accounts for about 95% of CAH
21 hydroxylase deficiency: Progesterone DOC: aldosterone Ø -severe hyponatremia -hyperkalemia hypotension -acidosis shock cardiovascular collapse death
21 hydroxylase deficiency: 17OHP II deoxycortisol: cortisol Ø • impairs postnatal carbohydrate metabolism • Exacerbates cardiovascular collapse (because a permissive action of cortisol is required for full pressor action of catecholamines)
21 hydroxylase deficiency: Cortisol ACTH • Adrenal hyperplasia stimulation of the transcription of the genes for all steroidogenic enzymes accumulation of non 21 hydroxylated steroids especially 17 OHP these steroids are converted to testosterone.
21 hydroxylase deficiency: • In the male fetus additional testosterone from the adrenals has little phenotypic effect • In the female fetus ovaries are quiescent-testosterone from the adrenals cause varying degrees of virilization of the external genitalia mild cliteromegaly ± posterior fusion of the labioscrotal folds complete labioscoral fusion + a urethra traversing the enlarged clitoris (I-V staging system of PRADER) • Ambiguous external genitalia + normal ovaries, Fallopian tubes and uterus or they appear to be male.
21 hydroxylase deficiency: • Diagnosis suggested by genital ambiguity in females, a salt-losing episode in the either sex, rapid growth in either sex, virilization in males • Plasma 17 OHP markedly elevated and hyperresponsive to stimulation with ACTH. Measurements: II-deoxycortisol DHEA, androstenedion
17OHP 17OHP assessments should not be made in the first 24h of life. Premature infants and term infants under severe stress may have elevated 17-OHP. 3ß HSD – P450cII deficiences
21 hydroxylase deficiency: Clinical forms of 21OHD: Classical Salt-wasting 21OHD: Due to complete deficiency of P450c21 activity (inappropriately large doses result in growth loss. Female survivors may have sexual dysfunction, marry with a low frequency and have decreased fertility.)
Simple virilizing 21 OHD: Males: • often escape diagnosis until age 3-7 years • testes remain of pre-pubertal size in CAH. • growth rapid-tall for age- bone age advances final height compromised • untreated or poorly treated children may fail to undergo puberty • azospermia – small testes
Treatment begun at several years of age: Suppression of adrenal testosterone secretion may remove tonic inhibition of the hypothalamus true central precocious puberty. Poorly treated boys enlargement of adrenal rests in the testes – (enlarged nodular testes.)
Non-classic 21OHD variant of normal? • premature development of pubic and axillary hair (premature pubarche) late onset CAH • Mild to moderate hirsutism • Virilism • Menstrual irregularities • Decreased fertility
No phenotypic manifestations but i.v. ACTH adm. results in an increased response of plasma 17 OHP. Cryptic CAH + mild impairment in mineralocorticoid secretion
21 hydroxylase deficiency: Incidence: Classic CAH : 1/14 000 Non-classic CAH: 1/100
21 hydroxylase deficiency: 21 hydroxylase genes: two 21hydroxylase loci CYP21A2 functional gene(microsomal cytochrome P450) CYP21AIP pseudogene