Download
1 / 16
170 likes | 709 Views
Tumor Localization Techniques. Richard Kao April 10, 2001 Computer Integrated Surgery II. Current Oncology Research. Tumor Localization Pre-operative localization techniques that provide the greatest accuracy before irradiating the lesion area Prevent tumor extension after treatment.

E N D
Tumor Localization Techniques Richard Kao April 10, 2001 Computer Integrated Surgery II
Current Oncology Research • Tumor Localization • Pre-operative localization techniques that provide the greatest accuracy before irradiating the lesion area • Prevent tumor extension after treatment
Definitions • Clinical Target Volume (CTV) • Area to be irradiated, built from 3-D imaging modalities • Delineation • Outlining the area of the tumor, including providing a perimeter to prevent tumor extension
Three Techniques • CT and/or MRI • Hookwire Localization • Bioimpedance
Papers • Jansen, E. et al. “Target volumes in radiotherapy for high-grade malignant glioma of the brain.” Radiotherapy and Oncology, vol. 56, pp. 151-156, 2000. • Sato, M. et al. “Laparoscopic hepatic surgery guided by hookwire localization.” 2000. • Lee, B. et al. “Bioimpedance: Novel Use of a Minimally Invasive Techniques for Cancer Localization in the Intact Prostrate.” The Prostrate, vol. 39, pp. 213-218, 1999.
CT • Computerized Tomography (CT) • Provides geometric superiority • 2-cm margin of error after postmortem analysis • Radiation
MRI • Magnetic Resonance Imaging (MRI) • Provides diagnostic superiority • 2-3 cm margin of error after postmortem analysis • Availability and costs
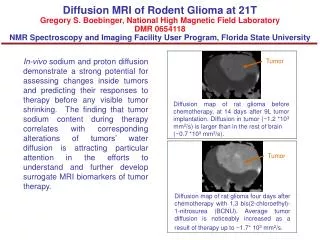
Jansen’s Findings • Patients had high-grade malignant astrocytoma, most common primary brain tumor • Found a lack of uniform guidelines • Discrepancy between tumor extension and CT and/or MRI results • Trade-off between probability of complications and the expected benefit for the patient • Had to add a 2-cm ring around images
Jansen’s Findings (cont.) • CT and MRI separately provide good information on both macro- and microscopic tumor extension • Ideal situation is to use both • For CTVs less than 250 cm3, use single CTV • For larger tumors, use a second TV with a smaller margin of irradiation
Sato’s Findings • Patients with small Hepatocellular Carcinomas (HCCs) • Helical and angiographic CT used to locate these lesions • Use CT to guide a 21-gauge guide needle to the lesion, then insert a hookwire through needle and withdraw the needle, leaving hookwire in place
Hookwire Localization • CT used to confirm hookwire in place • Microwave Coagulation Therapy (MCT) on HCCs • Complete tumor ablation • Radiation
Bioimpedance • Electrical property of biological tissue • Electric current is limited in living tissue by highly insulating cell membranes • Different tissue architecture may impede current differently, allowing detection of differences between normal and cancerous tissue
Lee’s Findings • Prostrate cancer diagnosed by transrectal ultrasound-guided sextant needle biopsy • Imprecise method • Use two bioimpedance needles 1 mm apart, 3 mm into prostrate surface
Lee’s Findings (cont.) • Cancerous areas had higher impedance (932 + 170 ohms) • Non-cancerous tissue had lower impedance (751 + 151 ohms) • Bioimpedance successful but still invasive and imprecise for different types
Conclusions • CT with MRI is effective but brings up questions regarding radiation and availability • Hookwire Localization requires CT scans both pre- and postoperation • Bioimpedance successful, but invasive and not appropriate for all types of tumor localization
Conclusions (cont.) • Using amorphous wires and magnetic fields to implement the Barkhausen effect, we provide a precise, reliable alternative that is readily available • Avoid pitfalls of these other techniques • Applicable to more areas than tumor localization, including catheter tip location, seed implants in brachytherapy, and probe tip location in surgical procedures