Download
1 / 17
210 likes | 514 Views
CMV (Cytomegalovirus) reactivation and immunosupression in allogeneic transplantation. Marie Waller Bone Marrow Transplant Coordinator Manchester Royal Infirmary. Aim. Introduction Quick overview of CMV Quick overview of CMV reactivation CMV reactivation risk groups

E N D
CMV (Cytomegalovirus) reactivation and immunosupression in allogeneic transplantation Marie Waller Bone Marrow Transplant Coordinator Manchester Royal Infirmary
Aim • Introduction • Quick overview of CMV • Quick overview of CMV reactivation • CMV reactivation risk groups • Quick overview of Immunosupression • How we monitor CMV at MRI • Treatment and management at MRI
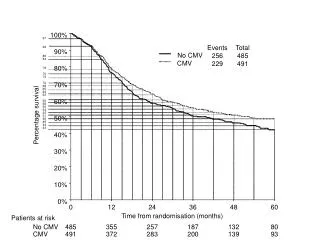
Introduction • Patients who have undergone allo HSCT are at risk of CMV reactivation • The use of immunosuppression is a recognised contributing factor in CMV reactivation • Treatment for CMV reactivation can be quite toxic and myelosuppressant • These patients may need higher levels of support, intervention, inpatient stay and nursing care • Before effective treatment strategies CMV reactivation had a high mortality rate of up to 90% from CMV pneumonitis
Cytomegalovirus (CMV) • Cytomegalovirus (CMV) is a common virus which is part of the herpes family • Once a person is infected with CMV, it will remain inactive for the rest of their life • Patients are at risk of CMV reactivation if they or the donor have had previous exposure to the virus • CMV causes few symptoms in most people • CMV infections occur mainly early in life • Low risk of transmission of CMV in transfused blood products
Cont • Once exposed to CMV virus you will develop detectable antibiotics (IgG) in your immune system • Approximately 30 - 90% of immunocompetent adults >40 years old have antibodies (IgG) to CMV, and are described as having positive CMV serology • In otherwise healthy adults, CMV remains inactive or latent • CMV can/ will become ‘active’ under favourable conditions
CMV reactivation • Once patients have been immunosuppressed they can have reactivation of CMV • This can result in invasive CMV disease such: pneumonitis, esophagitis,encephalitis, hepatitis, pancreatitis, adrenalitis, gastritis, enteritis, colitis, and retinitis • CMV reactivation is and can be life threatening
cont CMV seropositive patients (CMV IgG pos pre transplant) can reactivate CMV virus due to previous exposure as they already have the antibodies in their immune system CMV seronegative patients (CMV IgG neg pre transplant) can activate a newly acquired or a primary CMV infection from the allogeneic donor. This is transferred infection from the seropositive donor
CMV risk groups Risk of reactivation dependant on patient and donor previous exposure to CMV Patient/ DonorRisk CMV neg/neg (low risk) CMV pos/pos (high risk) CMV neg/ pos (high risk) (30% chance of reactivation) CMV pos/neg (high risk) (no donor immunity) At MRI we do not routinely use CMV prophylaxis
Immunesuppression • All patients undergoing allogeneic transplant will be given drugs to suppress the immune system • Prepares the patients body/ immune system to accept the graft from the donor and prevent rejection • Prevents/ reduces the risk of graft versus host disease (Immune response of the donor derived T cells against recipient tissues)
Immunosuppression • Reduces the patients ability to fight infection • Allows the patients immune system to reactivate dormant infections/ viruses • Allows the patients immune system to activate newly acquired primary infections transmitted from the donor’s immune system
Immunosuppression Drugs commonly used in Haematological transplantation are: Campath- anti CD52 lymphocyte suppressor ATG (anti thymocyte globulin)- suppresses T cells Fludarabine- lymphocyte suppressor Methotrexate – T-lymphocyte suppressor Cyclosporin A- T-lymphocyte (predonimantly) MMF (Mycophenolate mofetil)- immunosuppressor Tacrolimus- immunosuppressor Steroids
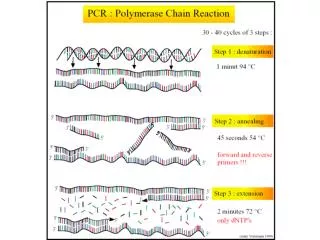
CMV monitoring • Viral reactivation can be monitored in different ways. PCR (polymerase chain reaction) is the most sensitive and readily quantifiable • Early treatment of low level reactivation reduces the risk of CMV infection progressing to clinically significant or organ disease • With the PCR method, CMV infection may be detected as early as two weeks before the onset of symptomatic CMV disease
Monitoring/ treatment at MRI • Following an SCT, CMV is monitored twice weekly using blood PCR (from Day 0) • Treatment initiated if 2 consecutive pos PCR results at or above limit of sensitivity • Treatment may be initiated on a single pos result if: • CMV disease proven or detected • High level reactivation ie log>3 • High risk cases (organ specific, high risk patient with multiple episodes, high index suspicion of CMV)
Monitoring at MRI If asymptomatic or low level reactivation we start oral treatment If symptomatic with low level or high level reactivation start IV treatment straight away Require 3 negative results before stopping treatment (IV treatment may be changed to oral once CMV responding until 3xneg) Pre-emptive treatment for rising titres important as therapy unlikely to be successful once clinical symptoms develop
Treatment Oral Valganciclovir 900mg bd IV Ganciclovir( 5mg/kg) (myelosuppressive) Foscarnet (nephrotoxic) CMV specific immunoglobulins Donor derived CMV specific cytotoxic lymphocytes (trial) Retinitis – ganciclovir eye drops
Notes • Always follow local guidelines and practices • Refer to SOP for CMV screening and treatment • Refer to EBMT guidelines • Discuss with colleague in virology if further treatment advice required