Download
1 / 32
320 likes | 610 Views
Immediate and complete revascularisation is required in multivessel disease patients presenting with STEMI - Contra. Mark de Belder The James Cook University Hospital Middlesbrough. Debating against Martin: Mission Impossible. Reaction on first meeting (listening to) Martin.

E N D
Immediate and complete revascularisation is required in multivessel disease patients presenting with STEMI- Contra Mark de Belder The James Cook University Hospital Middlesbrough
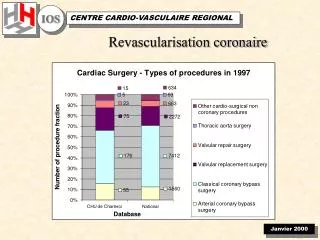
More multi-vessel procedures are being done (in elective patients and non-STEMI ACS) • Multi-vessel stenting in the era of DES and GP IIb/IIIa inhibitors is delivering outcomes comparable with CABG
Staged vs non-staged procedures in multivessel PCI(predominantly non-emergency)Nikolsky E et al, Am Heart J 2002;143:1017-26 * Staged procedure single independent predictor of lack of MACE at 1-yr (p=0.05)
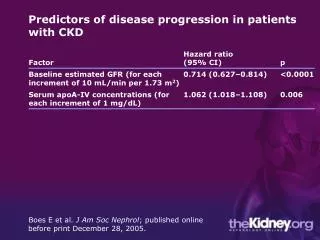
Multi-vessel disease in AMI • Multi-vessel disease occurs in 40-65% of patients with AMI • It confers higher risk in general and higher risk after intervention • PCI of the IRA is beneficial • The benefits of treatment of non-culprit vessels are unknown Kahn JK et al, JACC 1990;16:1089-96 Kahn JL et al, Am J Cardiol 1990;66:1045-8 Muller DW et al, Am Heart J 1991;121:1042-9 Jaski BE et al, Am Heart J 1992;124:1427-33 Shihara M et al, Am J Cardiol 2002;90:932-6 Keeley EC, Boura JA, Grines CL. Lancet 2003;361:967-8
The case for performing multi-vessel PCI during infarct angioplasty • Flow in non-IRA vessels is not normal and is worse in vessels with >50% stenosis • Slow flow in the non-IRA is associated with reduced non-IRA territory wall thickening, which improves when flow returns to normal • Enhanced function in the non-IRA territory confers a survival advantage • Patients often have multiple complex plaques • Coronary plaque instability can be a multi-focal process • These patients have higher event rates • Treatment of these unstable plaques may be beneficial • May be crucial in patients with cardiogenic shock • Simultaneous multi-vessel PCI may reduce vascular access and anti-coagulant related complications and reduce costs Grines CL et al. Circ 1989;80:245-53 Gibson CM et al, JACC 1999;34:974-82 Santoro GM, Buonamici P. Am Heart J 1999;138:126-31 Gregorini L et al, Circ 1999;99:482-90 Hochman JS et al, NEJM 1999;341:625-34 Goldstein JA et al, NEJM 2000;343:915-22 Asakura M et al, JACC 2001;37:1284-8 Hanratty CG et al, JACC 2002;40:911-6
“Costs” • Multi-vessel PCI is more costly to the provider • Staged PCI in the same hospital admission only attracts a single procedural cost • In the UK, commissioners currently pay a single price for PCI, regardless of complexity • Complex or staged procedures undoubtedly save “costs” for commissioners but are very expensive for providers
The case against performing multi-vessel PCI during infarct angioplasty • Every PCI for every lesion carries a finite risk • Non-culprit lesion severity is often exaggerated during AMI • State of vasoconstriction • Enhanced thrombotic and inflammatory state persists for some time after an AMI • Longer more complex procedures (contrast nephropathy, haemodynamic instability) • Additional time, more radiation exposure • Additional cost of the index procedure • Benefits not proven Fuster V et al. Circulation 1990;82:47-59 Shah PK, Forrester JS. Am J Cardiol 1991;68:16-23C Stewart DJ et al. JACC 1991;18:38-43 Hempel SL et al. Am J Physiol 1993;264:1448-57 Ambrose JA, Weinrauch M. Arch Intern Med 1996;156:1382-94 Haught WH et al. Am Heart J 1996;132:1-8 Reilly MP et al. Circulation 1997;96:3314-20 Bogaty P, et al. Am Heart J 1998;136:884-93 Bogaty P et al, Circ 2001;103:3062-8 Hanratty CG et al, JACC 2002;40:911-6 Barrett TD et al, J Pharmacol Exp Ther 2002;303:1007-13
Risk factors for contrast nephropathy • Pre-existing renal impairment • Congestive heart failure • Mitral regurgitation • Acute myocardial infarction • Dehydration • Gender (females>males) • Route of administration (I-A > I-V) • Diabetes? (probably dependent on co-existent renal damage) • Elderly? (ditto) • Concurrent use of NSAIDs and other nephrotoxic drugs • Widespread evidence of arterial disease • Hypotension • Hypoalbuminaemia
Which other lesion(s) should you treat?Patients with follow-up angiograms after infarct angioplastyHanratty CG et al, JACC 2002;40:911-6 • Vasoconstriction at time of STEMI more likely an explanation than plaque regression or haemodynamic factors • If immediate revascularisation were attempted on all lesions >50%, this would prompt unnecessary PCI in 1:5 patients
Multivessel PCI in infarct angioplastyRoe MT et al, Am J Cardiol 2001;88:170-3 • 79 cases collected from 8 centres of multi-vessel PCI during infarct angioplasty • 79 control cases of IRA only PCI in patients with multivessel disease (matched for age and Killip class) • Not confined to shock cases (only 28% Killip IV in both groups)
Multi-vessel PCI in infarct angioplastyRoe MT et al, Am J Cardiol 2001;88:170-3
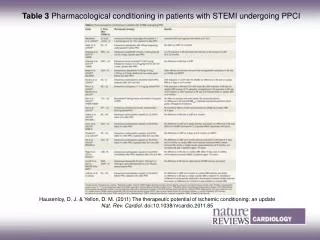
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600 • Patients undergoing staged procedures at a second admission excluded • *Defined as stenosis 70% of 2 epicardial vessels or their major branches • If stent, clopidogrel 75mg od x at least 4 weeks
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600 MV predictors of 1 yr mortality: Renal insufficiency, MV disease, EF≤40%, Age
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600Patients with multivessel disease MV analysis for1-yr MACE: MV PCI OR 1.67 (95%CI 1.10-2.54, p=0.01)
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600Multi-vessel procedures
Multi-vessel PCI in infarct angioplastyCorpus RA et al, Am Heart J 2004;148:493-600Conclusions • Patients with MVD have worse outcomes • Perform IRA PCI only • Decisions about other vessels should be guided by objective evidence of significant residual ischaemia • Further trials needed.
80 year old male in shock IABP inserted..
59 yr old male, anterolateral MI, D1 culprit ..but LAD and distal Cx? Which vessel?
Which vessel? 74 yr old male, anterior MI Reduced flow in LAD and intermediate Both acute? 1 chronic?
67 year old female, posterior MI Next day..
64 yr old male, 6m breathlessness, presents with infero-posterior STEMI 1 week later, wbc and CRP down
Should LAD be done? Asymptomatic, but 1-2mm ST depression on ETT 59 yr old male, inferior MI, FINESSE trial
Very well until 1 year later, non-STEMI 56 yr old male, inferior MI
66 yr old man, non-STEMI, 3VD, referred for CABG, then STEMI 3 days later
Conclusions • Cardiogenic shock is the one situation when it is generally accepted that multi-vessel PCI during infarct angioplasty might be helpful • Current evidence does not justify a protocol that mandates multi-vessel PCI in this setting • It may not be unreasonable in individual patients • Potential benefits must be weighed against the undoubted risks – the strategy overall may be harmful • A large randomised trial using up-to-date techniques is warranted (but will it ever be done?)
…and finally • Until then… • Do things because you should do them, not because you can! • Or, alternatively… • Just because you’ve got them, • don’t let them cloud your clinical judgement. • And keep them to yourself!