Download
1 / 12
130 likes | 271 Views
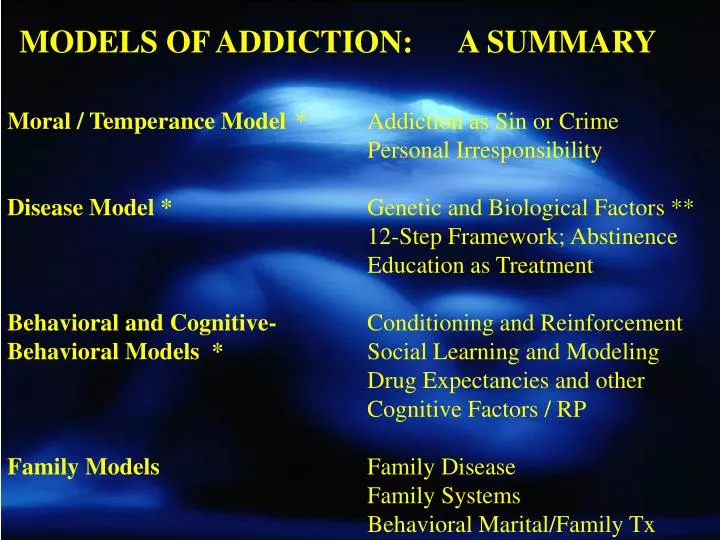
MODELS OF ADDICTION: A SUMMARY. Moral / Temperance Model * Addiction as Sin or Crime Personal Irresponsibility Disease Model * Genetic and Biological Factors ** 12-Step Framework; Abstinence Education as Treatment

E N D
MODELS OF ADDICTION: A SUMMARY • Moral / Temperance Model * Addiction as Sin or Crime • Personal Irresponsibility • Disease Model * Genetic and Biological Factors ** • 12-Step Framework; Abstinence • Education as Treatment • Behavioral and Cognitive- Conditioning and Reinforcement • Behavioral Models * Social Learning and Modeling • Drug Expectancies and other Cognitive Factors / RP • Family Models Family Disease • Family Systems • Behavioral Marital/Family Tx • Psychological / Psychoanalytic Disordered /Addictive Personalities • Sociocultural Models Cultural Factors • Socioeconomics/ Social Policy • Drug Subcultures • Public Health Model Agent, Host, Environment • Interactions • THE BIOPSYCHOSOCIAL MODEL: AN INTEGRATION • MODELS OF ADDICTION: A SUMMARY • Moral / Temperance Model Addiction as Sin or Crime • Personal Irresponsibility • Disease Model Genetic and Biological • Factors • 12-Step Framework; Abstinence, Education as Treatment • Psychological / Psychoanalytic Disordered /Addictive • Personalities • Behavioraland Cognitive- Conditioning and • Behavioral Models Reinforcement • Social Learning / Modeling • Drug Expectancies and other Cognitive Factors / RP • Family Models Family Disease • Family Systems • Behavioral Marital/Family • Therapy • Sociocultural Models Cultural Factors • Socioeconomic Factors • Drug Subcultures • Social Policy (e.g., drug control) • Public Health Model Interactions between • Agent • Host • Environment • THE BIOPSYCHOSOCIAL MODEL: • AN INTEGRATION
MODELS OF ADDICTION: A SUMMARY • Psychological / Psychoanalytic Disordered /Addictive Personality • Sociocultural Models Cultural Factors • Socioeconomics/ Social Policy • Drug Subcultures • Public Health Model Agent, Host, Environment • Interactions • THE BIOPSYCHOSOCIAL MODEL: • AN INTEGRATION
MODELS OF ADDICTION • Assumptions of Disease Model • addiction seen as a “primary” disease process • alcoholics qualitatively different from non • alcoholics: can’t drink in moderation • central symptom of addiction is loss of control • (e.g., one drink, one drunk) • addiction is chronic and progressive; no cure, • can only be arrested with total abstinence • (e.g. progression models - Johnson…learning & seeking the mood swing; harmful dependence; drinking to feel normal)
Disease Model - Treatment • Early identification • Education about diagnosis • Acceptance of disease and overcoming “denial” • Abstinence • 12-steps essential for real recovery
12 Steps of Alcoholics Anonymous 1. We admitted we were powerless over alcohol - that our lives had become unmanageable. 2. Came to believe that a Power greater than ourselves could restore us to sanity. 3. Made a decision to turn our will and our lives over to the care of God as we understoodHim. 4. Made a searching and fearless moral inventory of ourselves. 5. Admitted to God, to ourselves, and to another human being the exact nature of our wrongs.
12 Steps of AA (con’t) 6. Were entirely ready to have God remove all these defects of character. 7. Humbly asked Him to remove our shortcomings. 8. Made a list of all persons we had harmed and became willing to make amends to them all. 9. Made direct amends to such people wherever possible, except when to do so would injure them or others. 10. Continued to take moral inventory and when we were wrong promptly admitted to it.
12 Steps of AA (con’t) 11. Sought through prayer and meditation to improve our conscious contact with God as we understood Him, praying only for knowledge of His will for us and the power to carry that out. 12. Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics, and to practice these principles in all our affairs.
CRITIQUE OF DISEASE MODEL Strengths - perception shift: from sin to TX - eases guilt, self-blame - disease is a good metaphor that fits the experience - 12-step support and framework works for many (prevalence of meetings; 24-hour support…) - Other strengths? _______________________
Disease Model - Research Support • Adoption study of Goodwin • 18% probands alcoholic vs. 5% controls • Twin Studies • male vs. female twin pairs • Metabolic Studies • P3 Wave Studies
CRITIQUE OF DISEASE MODEL • Limitations • Assumptions not all data-based • addiction as “primary” • loss of control • chronic / progressive • alcoholics qualitatively different • - Dichotomous thinking dangerous; no middle ground (you’re an alcoholic or not) • - Loss of control and responsibility paradox • - Other flaws? ___________________
SUBSTANCE USE DISORDERS • GENERAL METHODS OF TREATMENT • Inpatient Detoxification and Rehabilitation • Outpatient Individual, Couple, or Family • Counseling • Self-help Groups (Alcoholics Anonymous; • NA, CA, OA, GA, Al-Anon etc.) • Residential Facilities & Therapeutic • Communities • Medications
Type of Treatment Goal of Treatment Description Frequency CBT (Cognitive Behavioral Therapy) Learn skills to achieve and maintain sobriety Coping and drink-refusal skills taught by therapist to handle states and situations known to precipitate relapse 12 weekly sessions TSF (Twelve Step Facilitation) Acceptance of the disease of alcoholism and loss of control over drinking Patients introduced by therapist to the first steps of Alcoholics Anonymous and encouraged to attend meetings 12 weekly sessions MET (Motivational Enhancement Therapy) Mobilize the person’s own commitment and motivation to change Therapist applies motivational psychology to examine effect of drinking on patient’s life, and develop and implement a plan to stop drinking 4 sessions in 12 weeks Project MATCH Treatment Conditions – Modalities You Will Learn