Download
1 / 5
60 likes | 227 Views
Patient repositioning and pressure ulcer risk—Monitoring interface pressures of at-risk patients. Matthew J. Peterson, PhD; Nikolaus Gravenstein, MD; Wilhelm K. Schwab, PhD; Johannes H. van Oostrom, PhD; Lawrence J. Caruso, MD. Aim

E N D
Patient repositioning and pressure ulcer risk—Monitoring interface pressures of at-risk patients Matthew J. Peterson, PhD; Nikolaus Gravenstein, MD; Wilhelm K. Schwab, PhD; Johannes H. van Oostrom, PhD; Lawrence J. Caruso, MD
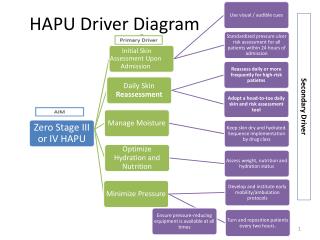
Aim • Examine the effect of routine repositioning over an extended time period on the interface pressures of the perisacral skin area of bedridden patients at risk for pressure ulcer formation using interface pressure mapping. • Relevance • Several recent studies in which repositioning was used as the primary intervention strategy failed to reduce the incidence of pressure ulcer formation .
Method • Used interface pressure mapping to assess how effectively routine repositioning relieves at-risk tissue of perisacral area. • Recorded perisacral skin-bed interface pressures of bedridden patients at risk for pressure ulcer formation every 30 s during routine repositioning care for 4–6 h.
Results • At-risk patients have skin areas that are likely always at risk throughout their hospital stay despite repositioning. • Skin areas that exceeded elevated pressure thresholds for >95% of observation period: • All participants (23): 206 ± 182 cm2. • Participants observed in supine, turned left, turned right positions (13): 166 ± 184 cm2.
Conclusion • Healthcare providers are unaware of actual tissue-relieving effectiveness (or lack thereof) of repositioning interventions. • May partially explain why pressure ulcer mitigation strategies are not always successful. • Relieving at-risk tissue is necessary part of pressure ulcer prevention, but repositioning practice itself needs improvement.