Download
1 / 24
260 likes | 499 Views
Pressure Ulcer Prevention at North Memorial. So what’s the big deal ?. Why We Practice Pressure Ulcer Prevention. Maintenance of skin integrity and pressure ulcer prevention is a nursing sensitive indicator of quality nursing care (American Nurses Association).

E N D
Why We Practice Pressure Ulcer Prevention • Maintenance of skin integrity and pressure ulcer prevention is a nursing sensitive indicator of quality nursing care (American Nurses Association).
Why We Practice Pressure Ulcer Prevention • It’s a community expectation.
Why We Practice Pressure Ulcer Prevention • Pressure ulcers are a reportable complication. • www.health.state.mn.us/patientsafety • Patient Safety Link • Adverse Health Events in Minnesota • Avoidable vs. Unavoidable
Why We Practice Pressure Ulcer Prevention • It is more cost effective to prevent a pressure ulcer than to treat one. • Average cost per ulcer = $27,000 • Annual US healthcare costs are over $3.6 billion
Why We Practice Pressure Ulcer Prevention • It’s the right thing to do !!!!
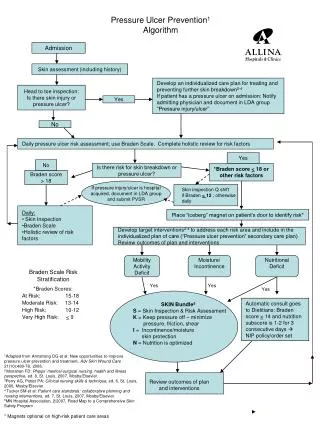
Components of a Pressure Ulcer Prevention Program • A clear process for identifying a patient's risk for developing pressure ulcers. • Strategies aimed at pressure ulcer prevention for the patient at risk.
Components of a Pressure Ulcer Prevention Program • Pressure ulcer prevention and treatment initiatives should be: • Evidence based • ICSI (Institute for Clinical Systems Improvement) Guidelines (2006) www.mnpatientsafety.org • WOCN Clinical Practice Guideline (2003). Prevention and Management of Pressure Ulcers. www.wocn.org • NPUAP (National Pressure Ulcer Advisory Panel) www.npuap.org
Risk Assessment • Should be performed at the point of entry to a health care facility and repeated on a regularly scheduled basis or with any change in condition. • At the time of patient "hand offs". WOCN Guideline for Prevention and Management of Pressure Ulcers (2003).
Intensity and duration of pressure Sensory perception Mobility Activity Tissue tolerance for pressure Moisture Nutrition Friction/shear Scoring 6-23 As scores become lower, predicted risk becomes higher. Mild risk: 15-18 Mod risk: 13-14 High risk: 10-12 Very high risk 9 or less Risk Assessment: Braden Scale
Peripheral Vascular Disease Myocardial Infarction Stroke Multiple trauma Musculoskeletal disorders GI bleed Bariatric Unstable and/or chronic medical conditions History of previous pressure ulcer Immunosuppression Preterm neonates Spinal cord injury Neurological disorders Risk Assessment: High Risk Groups
Risk Assessment: Skin Inspection • A head to toe inspection and palpation should be done on every patient upon admission, particularly over pressure points. • Repeat every 8-24 hours • Inspect • Palpate • Ask ICSI (2006)
Risk Assessment • Documentation • Communication • Patient Education
Skin Safety: Pressure Ulcer Prevention • Minimize or eliminate friction and shear. • Minimize pressure • Manage moisture • Maintain adequate nutrition/hydration
Skin Safety: Friction and Shear Friction: • The force of two surfaces moving across each other • Can cause superficial abrasions or blisters
Skin Safety: Friction and Shear Shearing Force: • Skin sticks to surface • Deeper tissues move in opposite direction • Capillaries kink • Local ischemia
Skin Safety: Minimize Pressure • Schedule regular and frequent turning and repositioning for bed and chair bound individuals. • Use support surfaces on beds and chairs to reduce or relieve pressure. • Relieve pressure to heels by using pillows or other devices.
Skin Safety: Manage Moisture Skin hydration issues • Dry skin • Skin with too little moisture 2.5 times more likely to ulcerate than healthy skin. • Skin moist from incontinence • 5 times more likely to ulcerate than dry skin.
Skin Safety: Manage Moisture • Implement a toileting schedule • Use ph-balanced cleansers • Contain urine or stool • Avoid chux, briefs, diapers.
Skin Safety: Maintain adequate nutrition and hydration • Maintain adequate nutrition that is compatible with the individual’s wishes or condition. • Consult a nutritionist in cases of suspected or identified nutritional deficiencies.
Skin Safety • Documentation • Communication • Patient/Caregiver Education • Causes and risk factors • Ways to minimize risk • Implementation
Is your process in place? • Risk assessment done on admission and at appropriate intervals? • Appropriate prevention strategies initiated for patients at risk? • Appropriate referrals initiated? • Patient/caregiver education done? • Document, document, document.