Download
1 / 17
170 likes | 493 Views
HORIZONS AMI. Effect of Switching Antithrombin Agents for Primary Angioplasty in Acute Myocardial Infarction The HORIZONS-SWITCH Analysis. Dangas G, et al JACC 2011;57:2309–16. Background and Methods.

E N D
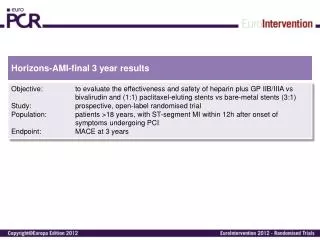
HORIZONS AMI Effect of Switching Antithrombin Agents for Primary Angioplasty in Acute Myocardial Infarction The HORIZONS-SWITCH Analysis Dangas G, et al JACC 2011;57:2309–16
Background and Methods • The safety and efficacy of switching anticoagulants in the early treatment of STEMI is unknown. • In the HORIZONS-AMI randomized trial, 65.4% of patients in HORIZONS -AMI received pre-randomization heparin • The subgroup of HORIZONS-AMI patients (n=2357) treated with heparin before randomization was analyzed according to subsequent assignment to bivalirudin (Switch group, n=1178) or to heparin plus GPI (Control group, n=1179). • Randomization was stratified according to pre-randomization UFH administration, therefore the present analysis reflects a stand-alone randomized comparison less subject to confounding than a nonrandomized subgroup analysis Dangas G, et al JACC 2011;57:2309–16
Results • Patients received heparin in a transfer facility (n=650), ambulance (n=876), the enrolling hospital (n=797), or multiple locations (n=37). • Most patients (n=1934) received a UFH bolus only, the rest received a bolus plus infusion (n=399) or infusion only (n=22). • The mean UFH bolus dose was 4,912 ±1,684 IU and 4,892 ± 883 IU in the switch versus control groups (p =0.72) • Study antithrombin was given in the cath lab to 85% of patients, and in the ED to15% of patients • The duration from pre-randomization UFH bolus to study drug initiation was 64 ± 61 min vs 59 ± 55 min in the switch vs control groups (p=0.05). • The mean baseline activated clotting time (ACT) levels were 205 ± 95 s vs 183 ± 85 s in the switch versus control groups (p<0.001). Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 30-day Outcomes P=0.0002 P=0.0001 P=0.007 P=0.18 30-day event rates (%) MACE= Major Adverse Cardiovascular Events (death, reinfarction, target vessel revascularization for ischemia, or stroke), NACE= Net Adverse Clinical Events (MACE plus non-CABG major bleeding) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year Outcomes P=0.01 P=0.06 P=0.0004 P=0.007 2-year event rates (%) MACE= Major Adverse Cardiovascular Events (death, reinfarction, target vessel revascularization for ischemia, or stroke), NACE= Net Adverse Clinical Events (MACE plus non-CABG major bleeding) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 30-day Outcomes P=0.48 P=0.001 P=0.04 P=0.002 30-day event rates (%) (Target Vessel Revascularization) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year Outcomes P=0.48 P=0.001 P=0.04 P=0.002 2-year event rates (%) (Target Vessel Revascularization) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year 30 Control Heparin plus GP IIb/IIIa (n=1179) 25.3% Switch to Bivalirudin alone (n=1178) 25 21.4% 20 Net Adverse Clinical Events (%) 15 10 30-day HR [95%CI] = 0.63 [0.49, 0.80] p <0.001 2-year HR [95%CI] = 0.81 [0.68, 0.96] p=0.01 5 0 0 3 6 9 12 15 18 21 24 Time (months) Net adverse clinical events = Death/MI/target vessel revascularization, stroke. non-CABG major bleeding. Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year 6 Control Heparin plus GP IIb/IIIa (n=1179) 5 Switch to Bivalirudin alone (n=1178) 4 3.8% Cardiac Mortality (%) 3 2.3% 2 30-day HR [95%CI] = 0.56 [0.32, 0.98] p=0.04 2-year HR [95%CI] = 0.61 [0.38, 0.99] p=0.04 1 0 0 3 6 9 12 15 18 21 24 Time (months) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year 16 Control Heparin plus GP IIb/IIIa (n=1179) 14 13.0% Switch to Bivalirudin alone (n=1178) 12 10 8.4% Major Bleeding (%) 8 6 4 30-day HR [95%CI] = 0.60 [0.46, 0.79] p <0.001 2-year HR [95%CI] = 0.63 [0.49, 0.81] p <0.001 2 0 0 3 6 9 12 15 18 21 24 Time (months) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch 2-Year 6 Control Heparin plus GP IIb/IIIa (n=1179) 5 Switch to Bivalirudin alone (n=1178) 4.3% 4 3.1% Stent Thrombosis (%) 3 2 30-day HR [95%CI] = 1.17 [0.68, 2.02] p=0.57 2-year HR [95%CI] = 0.73 [0.46, 1.15] p=0.17 1 0 0 3 6 9 12 15 18 21 24 Time (months) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch Group • 30-day outcomes by ACT at the start of PCI before bivalirudin administration Baseline ACT <200 s (n=637) median 158 s Baseline ACT ≥200 s (n=362) median 257 s p=0.59 p=0.78 p=0.65 NACE MACE Major Bleeding (non-CABG-related) ACT= Activated Clotting Time; MACE= Major Adverse Cardiovascular Events (death, reinfarction, target vessel revascularization for ischemia, or stroke), NACE= Net Adverse Clinical Events (MACE plus non-CABG major bleeding) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch Group • 30-day outcomes by ACT at the start of PCI before bivalirudin administration Baseline ACT <200 s (n=637) median 158 s Baseline ACT ≥200 s (n=362) median 257 s p=0.35 p=0.39 p=0.60 Mortality, All Cause Reinfarction Stent Thrombosis ACT= Activated Clotting Time Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch Group • 2-year outcomes by ACT at the start of PCI before bivalirudin administration p=0.36 Baseline ACT <200 s (n=637) median 158 s Baseline ACT ≥200 s (n=362) median 257 s p=0.76 p=0.32 NACE MACE Major Bleeding (non-CABG-related) ACT= Activated Clotting Time; MACE= Major Adverse Cardiovascular Events (death, reinfarction, target vessel revascularization for ischemia, or stroke), NACE= Net Adverse Clinical Events (MACE plus non-CABG major bleeding) Dangas G, et al JACC 2011;57:2309–16
HORIZONS-AMI Switch Group • 2-year outcomes by ACT at the start of PCI before bivalirudin administration Baseline ACT <200 s (n=637) median 158 s p=0.80 Baseline ACT ≥200 s (n=362) median 257 s p=0.72 p=0.79 Mortality, All Cause Reinfarction Stent Thrombosis ACT= Activated Clotting Time Dangas G, et al JACC 2011;57:2309–16
Limitations • Despite the randomized treatment assignment, this substudy of the HORIZONS-AMI trial should be considered exploratory and hypothesis-generatingdue to limited statistical power. • A switch strategy from UFH to bivalirudin vscontinuing UFH without a GPI was not tested. • However, previous studies showed that adding a GPI to UFH reduces mortality and reinfarction after primary PCI, and thus before the HORIZONS-AMI trial, 90% of patients with STEMI undergoing primary PCI were treated with UFH plus GPI.
Conclusions • STEMI patients who receive early treatment with UFH may be safely switched to bivalirudin, a strategy that results in reduced hemorrhagic complications and cardiac mortality and enhanced event-free survival compared with UFH continuation and initiation of a GPI Dangas G, et al JACC 2011;57:2309–16