Download
1 / 18
180 likes | 321 Views
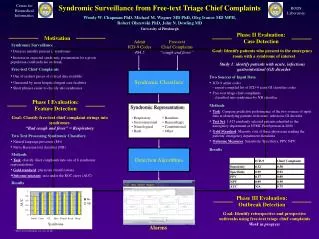
Results about Chief Complaints and OTC. Michael Wagner, MD PhD Real-time Outbreak and Disease Surveillance (RODS) Laboratory University of Pittsburgh. National Retail Data Monitor. OTC products have UPC bar codes Stores use optical scanners

E N D
Results about Chief Complaints and OTC Michael Wagner, MD PhDReal-time Outbreak and Disease Surveillance (RODS) LaboratoryUniversity of Pittsburgh
National Retail Data Monitor • OTC products have UPC bar codes • Stores use optical scanners • Nine national chains own >19,000 stores and they agreed to send daily sales data from their data warehouses • “Antidiarrheals” and 17 other surveillance categories • Health Department Use • 260+ accounts/39 States) • Raw data feeds: New York State, New York City, National Capital Area (MD, VA, DC), CDC, New Jersey, Georgia, Indiana… Wagner et al, Design of a National Retail Data Monitor, JAMIA, Sept. 2003;10(5) 409-20
RODS OPEN SOURCE DEVELOPERS! Monday 3:30-5:30 PM JEREMY ESPINO openrods.sourceforge.net • Emergency room triage personnel enter chief complaints routinely • The registration computer transmits chief complaints as HL7 messages to HL7 message routers, which can transmit to a health dept • Bayesian classifier assigns the chief complaint to “respiratory” or other syndrome category Health Department Use -Pennsylvania ~50 hospitals -Utah ~25 EDs and Urgent cares -Ohio 3 hospitals -Under development Michigan, Atlantic City Tsui et al, Technical Description of RODS: A Real-time Public Health Surveillance System, JAMIA, Sept. 2003;10(5) 399-408
Research Question 1 • Does the Bayesian classifier have any ability to detect patients with respiratory (or other relevant bioterrorism syndrome)?
Case Detection Accuracy of Bayesian Classifier vs. gold standard DOH Manual ED log review Answer There is information (Area under curve is not 0.5) There is noise For many syndromes of interest to bioterrorism, we can detect half the cases Next question: can we use an array of these noisy detectors to achieve accurate detection of outbreaks? Sensitivity, specificity and likelihood ratio positive (LR+) measurements for the CoCo classifier using the Utah Department of Health emergency department gold standard. CoCo Syndrome UDOH Syndrome Sensitivity Specificity LR+ Respiratory Respiratory infection with fever* 0.52 0.89 5 Gastrointestinal Gastroenteritis without blood 0.71 0.90 7 Encephalitic Meningitis / encephalitis 0.47 0.93 7 Rash Febrile illness with rash* 0.50 0.99 56 Botulinic Botulism-like syndrome 0.17 0.998 104 *Required documentation of fever in the patient record. Courtesy Per Gesteland, MD
Research Question 2 • Can we detect outbreaks by monitoring daily counts of “respiratory” (and other syndromes of interest to bioterrorism) produced by Bayesian classification of all ED visits in a region?
Detecting Respiratory Outbreaks by Monitoring Free-text Chief Complaints Hospital Pneumonia and Influenza Diagnoses Respiratorychief complaints SDs from Mean 7 Years Ivanov and Gesteland
Detection from CCs precede that from admissions by 23 days (95% CI 12-33) ICD-9s for gastroenteritis and rotavirus
Research Question 3 • Can we detect outbreaks by monitoring daily sales of “diarrheal remedies”? (…and other product categories related to the early symptomatic treatment of bioterrorism diseases)?
2001 Crypto in North Battleford, Saskatchewan … Precautionary water advisory issued on 4/23 Detectable peak on 4/2 in sales of over-the-counter diarrheal remedies
Cryptosporidium Outbreak: Milwaukee 3X increase in sales March 1 Public health awareness April 5, 1993 Proctor et al. Surveillance data for waterborne illness detection: an assessment following a massive waterborne outbreak of Cryptosporidium infection. Epidemiol Infect. 1998;120(1):43-54. ***Proctor et al. Surveillance data for waterborne illness detection: an assessment following a massive waterborne outbreak of Cryptosporidium infection. Epidemiol Infect. 1998;120(1):43-54.
Research Question 4 • How small of an outbreak can we detect?
Using Realistic Injects--Deriving Shape of Injects From Real Sales Data During a Real Outbreak Fit curve using expectation-maximization algorithm 4.6 std dev increase
False Alarm Rate=25% 10% 5% 2% Probability of Detection Detection Delay (days from start of inject) Average Detection Performance for a 4.6 SD North Battleford Perturbation into 500 U.S. Zip Codes X
Summary of Methods • Case detection • Outbreak detection • Retrospective studies of actual outbreaks • “Single disease” e.g., Influenza, Cryptosporidium • Seasonal (winter outbreaks) • Prospective • Injects Maximum validity, but rare Maximum validity, and answer question whether heretofore undetectable outbreaks can be detected, but expensive Very important for exploring “detectability”
Acknowledgements • Commonwealth of Pennsylvania • DARPA • AHRQ • Alfred P. Sloan Foundation • New York State Department of Health • NLM Fellowship support of Dr. Espino