Download
1 / 12
120 likes | 336 Views
AHLTA. Data Quality Management Course 10 February 2009. DHIMS Sustainment. Known Issues. New Issues Error Code 102 False Positives Update on Old Issues Duplicate Patients ADM Writeback Errors Signed encounters that have not synched to the CDR Inferred/missing SADRs.

E N D
AHLTA Data Quality Management Course 10 February 2009 DHIMS Sustainment
Known Issues • New Issues • Error Code 102 False Positives • Update on Old Issues • Duplicate Patients • ADM Writeback Errors • Signed encounters that have not synched to the CDR • Inferred/missing SADRs
Why Duplicate Patient Records • Unintended human error during patient registration • Typographic errors • Critical errors (EDI_PN, SSN, Last_Name) • Less critical errors (MIDDLE_Name, Gender, SPONSOR_SSN, etc.) • Inaccurate information from source • Workflow-induced data entry issues during patient registration • Time pressure • Multiple eligibilities • Pseudo-SSN • Automated errors • Person Identification Service (PIDS) “fetches”, etc.
Attention to detail at the MTF • Ongoing assessment of error generation mechanism • No new items to report (see next slide) • Manual process developed to correct errors • Teamwork effort of site and TMCI contract team • Currently on hold due to drug-allergy information cancellations • Fix to arrive for testing 2/13, estimate resume merges 2/20 • Automated error correction • Contract awarded in December, automatic merges should begin in March (assuming above fix is in place) • Clerical staff issues • Air Force study; clerical staff training on duplicate record causes • Error rate dropped from 25% to 15% • Limit number of people with access to registration
Major causes of duplicate patient records • If accessing the master patient index is slow, users will often create a record "to get the patient seen"; this produces a duplicate record. Commonly, though the wait is not usually long. • DEERS has a very rigid trait matching system, so a mis-type will fail to find the patient's record. If the user doesn't review his/her input to detect the error , he/she might create a new record, again, to "get the patient seen". • We are looking at purchasing a modern trait-matching service that will cut way down on this (time-line not determined yet) • If there is a significant enough difference between the patient's DEERS demographics and the data that is entered, DEERS may recognize the person as a new patient. • The prospective trait-matching service should eliminate this
Major causes of duplicate patient records (cont’d) • If the patient gives incorrect demographic information to the user (error, language barrier, nicknames, non-western-type names), the same will happen as noted in #3 on the previous slide. • Use of Pseudo-SSN's (will almost always result in duplicate record): • Not everyone whose care is documented in AHLTA has a SSN yet (e.g. newborns and foreign nationals), but DEERS requires one • The necessary workaround is to create a "pseudo-SSN", to be replaced with the correct one when one is issued • There are rules about what numbers to place where in order to show that it is a PSSN rather than a true one, but sometimes errors occur • Also, the MTF has to keep track of these patients in order to substitute the real number when it is available--doesn't always happen
AHLTA and Patient Merge… • Current manual process for merging duplicate records • Duplicate records are detected either by provider at point of care or by automated “comb” of MTF LCS; MTF creates Trouble Ticket(s) • TMCI (Tier 3) Triage group receives and manages all MHS trouble tickets • After investigation and verification that it is truly a merge issue the information is sent to DISA • DISA then combines the different records into one “KEPT” record • Automated identification and resolution • Automated system will find duplicates and resolve them • Current rate of duplicate record creation is about 18000/year • There are currently 1.3 million duplicates identified in CDR – automated system will clean up
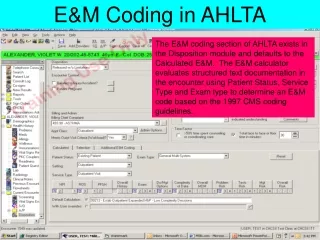
Error Code 102 Exceptions • ADM Processing Error - Failed WAM Validation • Invalid or Out-of-Sync ICD9 codes and CPT codes • 99371 is not a valid code value (99372,99373,99361,99362) • In addition have “False Positive” 102 errors (record appears in error report, but data is correct) during Oct/Nov 2008. • Error language is "at least 1 ICD9 code must be present" • This is fixed day forward but backlog is just now being cleared; No spreadsheet yet • There was a significant increase in EC 102 failures since March due to obsolete E&M codes being removed from the table without the replacement E&M codes being available for selection in AHLTA • These can be manually coded in CHCS by the site but they will still show on the AHTLA ADM exception report • We can have the site run an ad-hoc report in CHCS to confirm which failures were coded manually and change the status in the CDR so it will no longer be reflected as an EC 102 exception • This was remedied day-forward when all sites upgraded to 838.23. Fix of backlog is ongoing through NG Tier III • Backlog at all sites completed except: • Five sites have not sent in required information after 2 requests • One is still in process • 76% of the Oct EC 102 failures enterprise-wide are false positives failing with error: “At least 1 ICD9 code must be present”. This has been fixed day forward with the 3.3.3.1 mid-tier update 1 (3.3.3.2 MT) for all sites. NG will now work with sites to reset to 120. Encounters also need to be synched.
Error Code 103 Exceptions ADM Processing Error - Undefined CHCS Error Types of EC 103 errors Disposition is required Invalid Modifier MOD1 for EM code Injury Cause Code is missing M/Objects errors Enterprise Wide Problems (Fix is re-queue done centrally by NG) “Disposition is required”: Prior to the setting of the ADMp1p2 variable, CHCS/ADM was accepting the TCONS without dispositions (which is correct—the patient is not there). Afterward, the system required a disposition, with no method of entering one. Fix was implemented in November 2008 17 Sites have not sent in required information (after 2 requests) to NG for re-queue There is also a TCON error where there is no IEN Fix was implemented in November 2008 19 sites have not sent in required information after 2 requests Two sites await MObj 97 installation One site has cleanup in process
Signed encounters that have not synched to the CDR • These encounters are not seen on the ADM exception report even though there have been completed in AHLTA but not in CHCS • Problem fixed day-forward in Nov 08 but historical cleanup just now getting started; No progress spreadsheet available yet
Inferred/missing SADRs • Began increasing in January 2008 due to mismatch between FY 07 and FY 08 CPT codes • Steady decrease toward baseline since June 2008 due to implementation of the FY 08 CPT codes and NG re-queuing of the encounters