Download
1 / 23
300 likes | 894 Views
ATENEO SCHOOL OF MEDICINE AND PUBLIC HEALTH. CHRONIC COUGH. EVELYN VICTORIA E. RESIDE, MD., FPCP., FPCCP. Section of Pulmonary Medicine The Medical City. SESSION OUTLINE. Definition of terms Etiologies Burden of illness Diagnostic algorithm Summary. DEFINITION OF TERMS. ACUTE

E N D
ATENEO SCHOOL OF MEDICINE AND PUBLIC HEALTH CHRONIC COUGH EVELYN VICTORIA E. RESIDE, MD., FPCP., FPCCP. Section of Pulmonary Medicine The Medical City
SESSION OUTLINE • Definition of terms • Etiologies • Burden of illness • Diagnostic algorithm • Summary
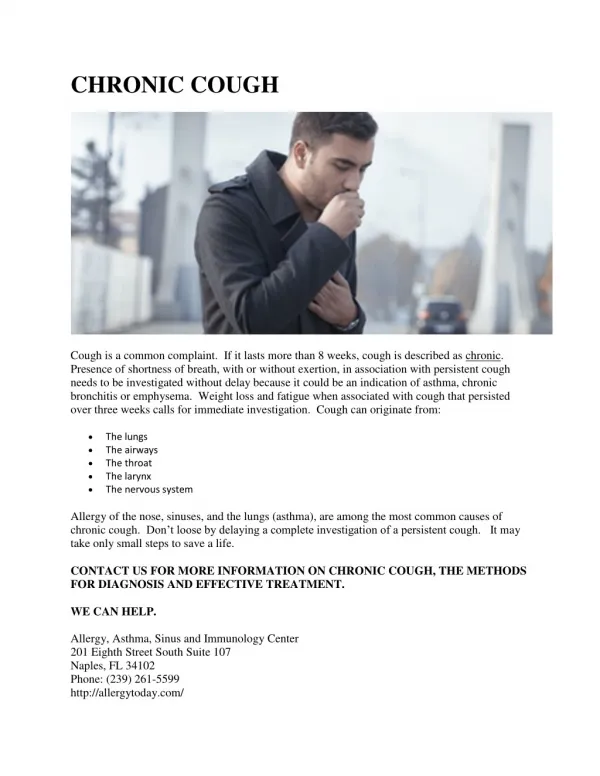
DEFINITION OF TERMS • ACUTE • < 3 weeks • SUBACUTE • Between 3 and 8 weeks • CHRONIC • > 8 weeks
DEFINITION OF TERMS • COUGH • A rapid expulsion of air from the lungs, typically in order to clear the lungs
ETIOLOGIES • Bronchial Asthma, Cough Variant Asthma • GERD or LPR • Postnasal Drip Syndrome or Chronic Upper Airway Cough Syndrome (UACS) • Pulmonary tuberculosis
DISEASE BURDEN • Among 284 cases seen: • Asthma 33.3% • UACS in 30.4% • PTB in 20.3% • GERD in 3.8%
May be due to • One condition 93% of the time • Two conditions 53% of the time • Three conditions 35% of the time • Four conditions 4% of the time
Clinical profile of patients with chronic cough due to asthma, UACS, GERD: • Patients complain of coughing • Patients are immunocompetent • Patients have a normal or near-normal chest Xray • Patients are nonsmokers and without significant environmental exposures • Patients are not taking an ace inhibitor
THE PHILIPPINE TASK FORCE ON CHRONIC COUGH THE UNIFIED ALGORITHM: Jennifer Mendoza-Wi, MD., FPCCP. Liza Llanes-Garcia, MD., FPCCP. Camilo Roa, MD., FPCCP. Abundio Balgos, Jr., MD., FPCCP Consuelo Obillo, MD., FPCCP. Rosauro Valenzuela, MD., FPCCP. Evelyn Victoria Reside, MD., FPCCP. With contributions from Dr. Richard Irwin (Immediate Past President, ACCP)
THE PHILIPPINE TASK FORCE ON CHRONIC COUGH CHRONIC UPPER AIRWAY COUGH SYNDROME: Zenaides Wi, MD., FPSO-HNS. Cesar Villafuerte, MD., FPSO-HNS. Joselito Acuin, MD., FPSO-HNS. WilliamLim, MD., FPSO-HNS. Madeleine Sumpaico, MD., FPSAII. Eileen Alikpala-Cuajunco, MD., FPSAII.
THE PHILIPPINE TASK FORCE ON CHRONIC COUGH BRONCHIAL ASTHMA: Liza Llanes-Garcia, MD., FPCCP. Dina Diaz, MD., FPCCP. Camilo Roa, MD., FPCCP.
THE PHILIPPINE TASK FORCE ON CHRONIC COUGH GASTROESOPHAGEAL REFLUX (GERD): Carla Sibulo, MD., FPSG. Gozaar Duque, MD., FPSG. Jaime Ignacio, MD., FPSG.
THE UNIFIED DIAGNOSTIC ALGORITHM Cough ≥ 2 weeks Normal CXR History of ACE-inhibitor intake, smoking & exposure to occupational irritants History and PE Stop ACE-inhibitor for 4 wks Smoking cessation Avoid exposure Cough gone Ace-Induced Cough Smokers’ cough Or Irritant cough NO YES
Cough gone Cough gone YES Treat as TB PTB Treatment Modification ON Hx of TB exposure NO YES YES AFB smears (+) Repeat Chest Radiograph PTB suspect 3 sputum AFB smears NO Initiate specific treatment NO Evaluate & treat for the Pathogenic Triad: (1) Asthma, (2) UACS and/or (3)GERD UACS, Asthma and/or GERD Response to treatment YES NO YES Optimize treatment and consider overlapping etiologies Cough gone NO
Repeat Chest Radiograph Normal CXR Post-infectious Cough or Psychogenic Cough YES Order according to likely clinical possibility Sputum cytology, HRCT scans, Modified BaE, Bronchoscopy, Cardiac Studies Treat Specific Conditions Accordingly
LET’S PLAY A GAME! WINNER: 10 POINTS 2ND PLACE: 9 POINTS 3RD PLACE: 8.5 POINTS 4TH PLACE: 8 POINTS
DIAGNOSTIC ALGORITHM FOR CHRONIC COUGH & GERD Chronic Cough Alarm Symptoms? Y GERD Symptoms Y N Y Empiric treatment with acid suppressants Y Continue treatment Improved? N Refer to Gastroenterologist
FLOW IN THE DIAGNOSIS OF CHRONIC COUGH & CHRONIC UPPER AIRWAY COUGH SYNDROME Chronic Cough and Possible Chronic Upper Airway Cough Syndrome History Physical exam Non-Allergic Rhinitis Rhinosinusitis Tonsillopharyngitis Laryngopharyngeal Reflux Allergic Rhinitis Diagnostics: Sinus Xrays, Sinus CT scan Therapeutics: Antibiotics, decongestants, mucolytics, surgery Diagnostics: History and Physical Exam Therapeutics: Antibiotics, surgery Diagnostics: Empiric therapy, 24-hr pH monitoring, Impedance measurement Therapeutics: Proton pump inhibitors Diagnostics: (+) Family history, response to empiric treatment, allergy skin tests Therapeutics: Environmental control, antihistamines, nasal steroids, immunotherapy, surgery
SUMMARY • History and PE ! • ACE inhibitor treatment and cigarette smoking • When dealing with acute cough, rule out life-threatening conditions, exacerbations of chronic illness or environmental/occupational exposure • Non-infectious causes of subacute cough are managed in the same way as chronic cough • Initial empiric treatment of chronic cough is a combination antihistamine + decongestant
SUMMARY • Stepwise approach towards the diagnosis • More than one etiology of cough can be present • If cough is due to ACE inhibitor intake, the drug should be stopped and replaced • If cough continues to persist, refer to a specialist!