Download
1 / 36
380 likes | 583 Views
Amoxycillin clavulanate in children with chronic wet cough. Journal Club Kavi Aucharaz 22.1.2014. Aim. To determine the efficacy of a 2 week course of Amoxycillin Clavulanate in the treatment of children with chronic wet cough . Case presentation.

E N D
Amoxycillinclavulanate in children with chronic wet cough Journal Club Kavi Aucharaz 22.1.2014
Aim To determine the efficacy of a 2 week course of Amoxycillin Clavulanate in the treatment of children with chronic wet cough
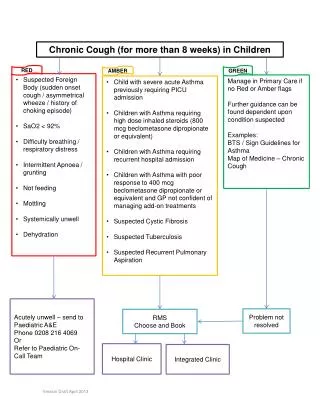
Case presentation 3 year old seen in AAU with a chronic wet cough for 5 months GP tried salbutamol and steroid inhalers no effect No audible wheeze Is it PBB and require prolonged course of antibiotics? Can we achieve cough resolution by treating chronic wet coughs with Amoxycillin clavulanate in children?
PBB-Protracted Bacterial Bronchitis • Defined as presence of isolated chronic wet cough • Resolution of cough with appropriate abx • Absence of an alternative cause for specific cough • Speculation that PBB maybe a precursor to chronic suppurative lung disease - left untreated
Current guidelines • Recommend abx for children with PBB • Advice based on a Cochrane review prospective and retrospective observational studies • Cochrane review of abx treatment for moist cough in children showed • Abx were effective • 1 clinical cure for every 3 children treated(95% CI 2 to 4)
Cochrane review • Based on 2 small studies of children with cough >10 days—not current definition • Current definition of chronic cough > 4 weeks • Neither study used validated outcome measures of cough • Parental reporting of cough in children is subject to bias
Placebo controlled RCT –Unicentre parallel study in Brisbane Double-blind RCT Aimed to assess efficacy of 2 weeks of oral amoxicillin clavulanate Compared with placebo in achieving cough resolution in children with chronic wet cough
Excluding criteria Inclusion criteria • Children aged 6mo-18 yrs • Newly referred to respiratory practice • Jan.2004- Dec 2006 • Chronic cough (> 3 wks)+ doctor observed moist/wet cough • Gross neuro-devlopmental delay • CF, Ex-prem (<37 weeks gest.) • Chr. Disease , interstitial lung disease or cardiac abn. • Suspicion of bronchiectasis • Haemoptysis • Abx therapy received in preceding 2 wks • Penicillin allergy/acutely unwell with fever or pnemonia
Randomisation and allocation • Computer generated • Stratified by age(<6yrs and >6yrs) • Parents and members of study were blinded to the child’s allocated group
Data collection • Standardised data collection sheets were used • Parents completed a daily cough diary for 28 days post enrolment --presence and severity of cough --any adverse reactions to medications were documented • Validated cough diary using the verbal category descriptive score (VCD) was used • Cough scoring system -- has best correlation with objective counts as measured by cough meter
Verbal Category Descriptive score(validated cough diary) 0=no cough 1=cough for one or two short periods only 2=cough for more than two short periods 3=frequent coughing but does not interfere with school and other activities 4=frequent coughing which interferes with school and other activities 5=cannot perform most activities due tp severe coughing
Child presenting to RCH with chronic (>3 weeks)cough Assess for eligibility and study explained to parents Clinical assessment : history, Physical exam±CXR Enrolled , randomised, diary prescription, diary cards explained Prescription taken to pharmacy Amoxicillin-clavulanate 22.5 mg/kg/dose twice daily(0.281ml/kg) Placebo twice daily(0.281 ml/kg) Day 7 review(phone) Day 14 review(phone) Routine clinical appointment arranged if still coughing Diaries and medication bottled received by post
Bronchoscopy Some children had flexible bronchoscopy Not a requirement of the protocol Children received the trial medication after the bronchoscopy BAL was performed –European Respiratory Society guidelines Microbiological exam. Cytology and inflammatory markers Significant bacterial growth ≥ 105 cfu/ml of BAL
OUTCOMES • Primary outcome ‘cough resolution’ • Defined as improvement in baseline cough score (>75% reduction of cough) • At ’end of trial’ or cessation of coughing for minimum 3/7 within trial period • Baseline cough score -- average score in the 2 days immediately before trial medication commencement • ‘End of trial’ score - the score 2 days following completion of 14 days of medication(D15-16) • Secondary outcome measure were absolute change in cough score and change in VCD score over the study
Statistical methods Sample size of 55-60 At 5% significance this provides a study power of 82% With 20-30% dropout rate to detect a difference of 60% between groups-(75% improvement in abx group,30% in placebo group) Without dropouts- sample size of 23 per group provided same power for the same effect size Dropout rate was low –study was ceased when 50 enrolled
Statistical analysis • Data were analysed with intention to treat • Children lost in F/U –considered failures • SPSS V.12 • Medians and IQR were used for descriptive data • Not normally distributed data were analysed using non-parametric analyses • Mann-Whitney U test used for comparisons b/w the 2 groups • Proportions between groups were compared using chi-squared test • Two tailed p value <0.05 considered significant
Results • 55 patients approached, 50 enrolled • 3 children lost to FU-unable to contact • All 50 children were included in final analysis • Similar no. in both arms had bronchoscopy(19,18) • BAL data - consistent with PBB in majority children • BAL microscopy identified • Haemophilus influenza(n=14. 34%) • Strep, pneumoniae(n=9, 24%) • Moraxella catarrhalis(n=7, 19%) • All these organisms were sensitive to Amoxycillin clavulanate
Assessed for eligibility N=55 Excluded(n=5) Decline to participate(n=3) Not meeting inclusion criteria(n=2) Randomised (n=50) Allocated to Abx(n=25) Received allocated intervention(n=25) Allocated to placebo(n=25) Received allocated intervention(n=25) Lost to follow-up(n=1) [reasons: unable to contact(n=1)] Discontinued interventions(n=0) Lost to follow up(n=2) [reasons :unable to contact(n=2)] Discontinued intervention(n=1) • Analysed for cure(n=25) • Secondary outcomes: • Excluded from analyses requiring cough scores(as none available)(n=2) • Bronchoscopy data;(n=19) • Analysed for cure(n=25) • Secondary outcomes: • Excluded from analyses requiring cough scores(as none available)(n=1) • Bronchoscopy data(n=18)
Effect of intervention Amoxycillinclavulanate group – more likely to achieve cough resolution (n=12, 48%) v/s Placebo group (n=4, 16%) (p=0.015) Observed difference between proportions is 0.32 (95%CI 0.08-0.56) OR=4.85
P- Children (6mo-<18ys) with chronic wet cough I- 2 weeks course of Amoxycillinclavulanate in treatment of chronic wet cough C-Placebo O- ‘Cough resolution’-defined as a<75 % reduction in validated VCD cough score • Randomisation was computer generated • Concealed allocation was used • Allocation list and trial medications were dispensed by pharmacy • Parents and members of study were blinded until data were analysed.
55 patients approached • 50 were enrolled and all received treatment allocation • 3 lost to follow up—unable to be contacted • All 50 children were included in the final analyses for primary outcome
Is it worth continuing?? …Yes • Parents and members of the study were blinded to allocated group until data were analysed • Medication code were revealed in February 2011 • Similar numbers (n=25) in both study arms
No significant difference between groups in • any of parameters • Similar number in both arms had bronchoscopy prior treatment commencement
Primary outcome was ’cough resolution’ • Defined as improvement in baseline cough score (>75% reduction in cough score) at ‘end of trial’ or cessation of coughing for minimum period of 3/7 within the trial period • Baseline cough score was children with chronic wet cough with a number need to treat –NNT (for benefit at 2 weeks) of 4
Observed difference between proportions is 0.32(95% CI 0.08-0.56) • OR=4.85, NNT for benefit at 2 weeks was 4 (95% CI 2 to 27) • At 4 weeks further 2 children were cough free (n=14, 56%)
Population are similar to Brisbane • Study period Jan 2004-Dec 2006 • Both summer and winter period
10/13(77%) in treatment group grew significant bacteria on BAL • Side effects were seen in both groups with no significant difference
Re-attendance at GP • Substantial amount of burden-family-Impact on QoL • The definition of chronic wet cough is different currently in UK(4-6wks) Tablets 375 mg, f/c, co-amoxiclav 250/125 (amoxicillin 250 mg as trihydrate, clavulanic acid 125 mg as potassium salt), net price 21-tab pack = £4.19. Label: 9 Tablets 625 mg, f/c, co-amoxiclav 500/125 (amoxicillin 500 mg as trihydrate, clavulanic acid 125 mg as potassium salt). Net price 21-tab pack = £8.00. Label: 9 Suspension ‘125/31 SF’, sugar-free, co-amoxiclav 125/31 (amoxicillin 125 mg as trihydrate, clavulanic acid 31.25 mg as potassium salt)/5 mL when reconstituted with water. Net price 100 mL (raspberry- and orange-flavoured) = £2.95. Label: 9 Suspension ‘250/62 SF’, sugar-free, co-amoxiclav 250/62 (amoxicillin 250 mg as trihydrate, clavulanic acid 62.5 mg as potassium salt)/5 mL when reconstituted with water. Net price 100 mL (raspberry- and orange-flavoured) = £3.00. Label: 9
Limitations of study Lack of follow up over period of months to assess long term value of 2 week antibiotic therapy Long delay between completion of study and data analyses Due to personal reasons of primary author
Summary and Conclusion VERY WELL DESIGNED STUDY AmoxycillinClavulanate is effective in achieving a reduction in symptoms and cough resolution in significant number of children with isolated chronic wet cough
Following Discussion No local guidelines at SCH for treatment of chronic wet cough It was felt that the long term effect of the 2 weeks course of oral antibiotics were not measured We do not know whether the chronic wet cough resolution was sustained for longer period Treating children having 3 weeks of wet cough with 2 weeks antibiotics is not justified. There is no concrete evidence to prove that untreated PBP leads to chronic suppurative lung disease