Download
1 / 28
320 likes | 721 Views
ANEMIA IN PREGNANY AND ROLE OF PARENTERAL IRON THERAPY. Dr SUSANTA KUMAR BEHERA SENIOR RESIDENT DEPARTMENT OF O & G MKCG MEDICAL COLLEGE BRAHMAPUR, ODISHA; INDIA. Most Common Nutritional Disorder in the World Incidence = 40 to 60 % of pregnant women in India

E N D
ANEMIA IN PREGNANY AND ROLE OF PARENTERAL IRON THERAPY Dr SUSANTA KUMAR BEHERA SENIOR RESIDENT DEPARTMENT OF O & G MKCG MEDICAL COLLEGE BRAHMAPUR, ODISHA; INDIA
Most Common Nutritional Disorder in the World • Incidence = 40 to 60 % of pregnant women in India • Commonest Medical(hematological) disorder during pregnancy • 25% of direct maternal deaths • Responsible for 40% of maternal deaths in third world countries. • India contributes to 80% of maternal deaths due to anemia in South Asia
Pregnancy : Most dangerous journey of mankind Anemia begins in childhood, worsens during adolescence in girls and gets aggravated during pregnancy
Quantitative or qualitative reduction of Hb or circulating RBC’s or both resulting in a reduced oxygen carrying capacity of blood to organs and tissues • Woman Hct 33% or Hb 11g/dl – 1st & 3rd trimester and Hct 32% or Hb 10.5 g / dl in 2nd trimester(CDC/WHO)
COMMON ANEMIAS IN PREGNANCY Physiological Acquired Nutritional deficiency anaemias - Iron deficiency (90%) - Folate deficiency - Vit. B12 deficiency • Infections : Malaria/Hookworm/UTI Hemorrhagic –acute/chronic blood loss • Bone marrow- Aplastic anemia • Renal diseases Genetic/Haemoglobinopathies: - SCD • - Thalassaemias
Plasma volume 50% (by 34weeks) but RBC mass only 25% • Disproportionate increase in plasma vol, RBC vol. and hemoglobin mass during pregnancy CRITERIA FOR PHYSIOLOGICAL ANAEMIA • Hb = 10 gm% • RBC = 3.2 million/mm3 • PCV = 30% • Peripheral smear showing normal morphology of RBC with central pallor
IRON REQUIREMENTS DURING PREGNANCY • Maternal req. of total Iron -1000mg • 500 mg Maternal Hb. Mass expansion • 300 mg Fetus & Placenta • 200mg Shed through gut., urine & skin • 2.5mg /day in early pregnancy • 5.5mg /day from 20 -32 weeks Average 4 mg/ day • 6 – 8 mg/ day after 32 weeks • Increases from 1-2mg in 1st trimester to 6-8 mg in 3rd trimester
Absorption of iron depends upon Amount of iron in the diet Bioavailability of iron Physiological requirements Iron sources are two types Haem iron(5%) : hemoglobin and myoglobin from red meat, poultry and fish Nonhaem iron(95%): fibers, green vegetables
NORMAL IRON CYCLE Duodenum Dietary iron (average, 1 - 2 mg Utilization Utilization per day) Plasma (TIBC) transferrin (3 mg) Bone Muscle marrow (myoglobin) (300 mg) Circulating (300 mg) erythrocytes Storage (hemoglobin) iron (Ferritin) (1,800 mg) Sloughed mucosal cells Desquamation/Menstruation Other blood loss (average, 1 - 2 mg per day) Reticuloendothelial Liver macrophages (1,000 mg) Iron loss (600 mg)
EFFECTS OF ANAEMA IN PREGNANCY ANTEPARTUM • Pre eclampsia • Intercurrent infection • Cardiac failure • Preterm labour • APH • PIH INTRAPARTUM • PPH • Cardiac failure • Shock • POSTPARTUM • Puerperal sepsis • Subinvolution • Failing lactation • Puerperal venous thrombosis • Pulmonary embolism
Baby IUGR Prematurity Increased risk of IDA early infancy Still births Congenital malformations ↑ in Neonatal deaths/Perinatal mortality Intra uterine deaths(severe maternal anoxemia) Abnormal Social and Emotional behaviour EFFECT OF PREGNANCY IN ANAEMIA Pt. Mildly anemic progresses to marked Anaemia Pt. Who is severely anemic becomes symptomatic by the end of 2nd trimester
IDA IN PREGNANCY Grandmulti Hook worm infestation Blood loss : Menorrhagia 20-30% Increase demand for iron particularly in 2nd & 3rd trimester Higher risk with morning sickness Aspirin/NSAIDS Multiple pregnancies Intolerance for red meat Low dietary intake (Vegetarians, Vit. C & Calcium) Malabsorption (Hypo-or achlorohydria) Losses can increase with colorectal cancer, polyps
STAGES OF IRON DEFICIENCY Prelatent(Depletion) : • Stores are depleted without a change in hematocrit or serum iron levels . • Reduced stored iron e.g. serum ferritin with normal hemoglobin Latent(iron deficient erythropoisis) : • Serum iron drops and the TIBC increases without a change in the hematocrit. • Reduced stored and transport iron • Increased erythrocyte protoporphyrin concentration • Detected by a routine check of the transferrin saturation.
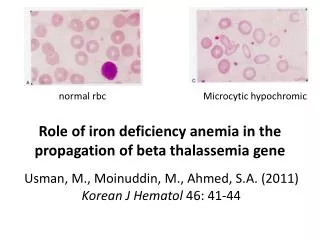
Frank IDA : • Associated with erythrocyte microcytosis and hypochromia. • Stage of deficiency of stored, transport and functional iron • Reduction of hemoglobin and serum ferritin • Low serum transferrin saturation • Increased erythrocyte protoporphyrin concentration • Iron deficiency attracts medical attention most commonly at this stage.
CLINICAL FEATURES • SYMPTOMS • Fatigue • Weakness • Headache • Loss of appetite • Dysphagia • Palpitations • Dyspnea on exertion • Ankle swelling • Paresthesia • Leukoplakia • Cold intolerance • irritability • SIGNS • Glossitis • Stomatitis • Heart murmurs • Increased JVP • Tachycardia • Tachypnea • Postural hypotension • Pallor • Dryness or roughness of the skin • Koilonychia • Dry & cracked lips & Brittle hair
DIAGNOSIS OF IDA • Low hemoglobin • Low serum ferritin<15 mcg/dl • Microcytic & hypochromic in absence of chronic diseases/hemoglobinopathies • Low serum iron content(< 30mcg/dL) • Low PCV, MCV, MCH, MCHC • High TIBC > 400 mcg/dl
Increased ZPP (>40 mmol/mole heme) • Low transferrin saturation(<15%) • Increased serum transferrin(>350mg/dL) • Increased serum soluble transferrin binding receptors(> 8 mg/L) • increased serum neopterin concentration
INVESTIGATIONS • Haematocrit • RBC Indices: - Low MCV - Low MCH - Low MCHC - Low PCV • Peripheral blood • Urine for haemturia(R&M/C&S) • Stool examination • Hb electrophoresis • X-ray Chest(PA View)
Serum iron < 50 μgm/dl • TIBC is increased - > 400 μgm/dl • Serum ferritin is < 12 μgm/dl • Serum transferrin saturation<20% • Red cell Zinc Protoporphyrin • Stainable iron in the bone marrow is reduced-Gold Standard • Serum transferrin receptor(TfR) : Increased • Bone marrow examination. • Reticulocyte hemoglobin conc. : Count of <26pg/ cell • LFT, RFT • Trial of iron therapy-diagnostic & therapeutic
TREATMENT • Anaemicgravidas 120 –240mg / per day • Supplementation with folic acid + Vit C. • Ferrous sulphate 300mg TID daily after meals X 12 months • Therapeutic results after 3 weeks – rise in Hb % level of 0.8gm/dl/ week with good compliance • Rise in Hb at a rate of 2-4 gm/dl every 3 weeks till normal • Hb conc. is normal after 6 wks of therapy
INDICATORS OF IRON THERAPY RESPONSE • Increase in Reticulocyte count (Increases 3-5 days after initiation of therapy ) • Increase in Hb levels. Hb increases 0.3 to 1 g/ week • Epithelial changes (esp tongue & nail ) revert to normal
Pregnancy >36wks Pregnancy <30wks Pregnancy 30-36wks IDA FA def. Oral iron Oral FA Intolerance or Non-compliance I/M iron I/V iron IDA FA def. ParenteralOral FA I/M iron I/V iron Blood transfusion
ORAL IRON THERAPY WHO : 60 mg elemental iron + 250 ug FA OD/BD. Govt. of India : 100 mg Fe + 500 ug FA during 2nd half of pregnancy X 100 days. Drawbacks: - Intolerance - Unpredictable absorption rate. - Not suitable for patients with GI diseases/ significant bleeding - Non Compliant patient. - Long time for improvement
Side effects • Nausea & Vomiting • Gastric irritation • Constipation • Abdominal cramp • Diarrhoea Response to therapy: - Sense of well being/Increased appetite. - Increase in Hb approximately 2gm% per every 3-4 wk - Reticulocytosis with in 5-10 days - hematocrit returning to normal .
Interesting, right? This is just a sneak preview of the full presentation. We hope you like it! To see the rest of it, just click here to view it in full on PowerShow.com. Then, if you’d like, you can also log in to PowerShow.com to download the entire presentation for free.