Download
1 / 1
10 likes | 195 Views
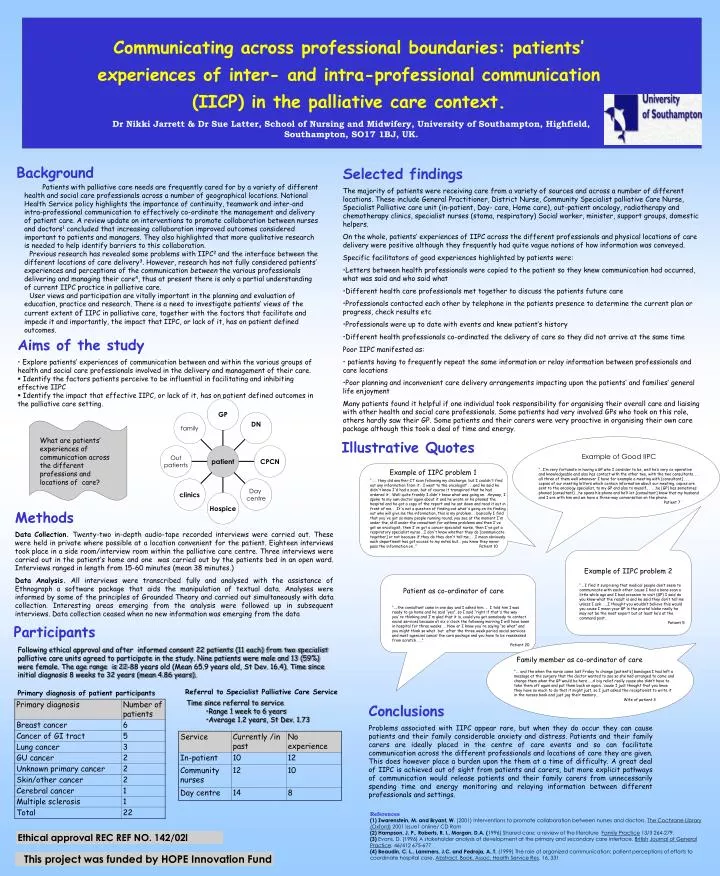
Communicating across professional boundaries: patients’ experiences of inter- and intra-professional communication (IICP) in the palliative care context . Dr Nikki Jarrett & Dr Sue Latter, School of Nursing and Midwifery, University of Southampton, Highfield, Southampton, SO17 1BJ, UK. .

E N D
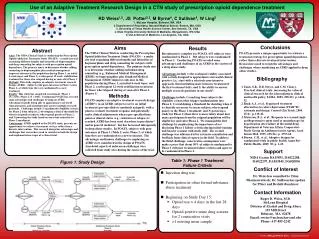
Communicating across professional boundaries: patients’ experiences of inter- and intra-professional communication (IICP) in the palliative care context. Dr Nikki Jarrett & Dr Sue Latter, School of Nursing and Midwifery, University of Southampton, Highfield, Southampton, SO17 1BJ, UK. • Background • Patients with palliative care needs are frequently cared for by a variety of different health and social care professionals across a number of geographical locations. National Health Service policy highlights the importance of continuity, teamwork and inter-and intra-professional communication to effectively co-ordinate the management and delivery of patient care. A review update on interventions to promote collaboration between nurses and doctors1 concluded that increasing collaboration improved outcomes considered important to patients and managers. They also highlighted that more qualitative research is needed to help identify barriers to this collaboration. • Previous research has revealed some problems with IIPC2 and the interface between the different locations of care delivery3. However, research has not fully considered patients’ experiences and perceptions of the communication between the various professionals delivering and managing their care4, thus at present there is only a partial understanding of current IIPC practice in palliative care. • User views and participation are vitally important in the planning and evaluation of education, practice and research. There is a need to investigate patients’ views of the current extent of IIPC in palliative care, together with the factors that facilitate and impede it and importantly, the impact that IIPC, or lack of it, has on patient defined outcomes. • Selected findings • The majority of patients were receiving care from a variety of sources and across a number of different locations. These include General Practitioner, District Nurse, Community Specialist palliative Care Nurse, Specialist Palliative care unit (in-patient, Day- care, Home care), out-patient oncology, radiotherapy and chemotherapy clinics, specialist nurses (stoma, respiratory) Social worker, minister, support groups, domestic helpers. • On the whole, patients’ experiences of IIPC across the different professionals and physical locations of care delivery were positive although they frequently had quite vague notions of how information was conveyed. • Specific facilitators of good experiences highlighted by patients were: • Letters between health professionals were copied to the patient so they knew communication had occurred, what was said and who said what • Different health care professionals met together to discuss the patients future care • Professionals contacted each other by telephone in the patients presence to determine the current plan or progress, check results etc • Professionals were up to date with events and knew patient’s history • Different health professionals co-ordinated the delivery of care so they did not arrive at the same time • Poor IIPC manifested as: • patients having to frequently repeat the same information or relay information between professionals and care locations • Poor planning and inconvenient care delivery arrangements impacting upon the patients’ and families’ general life enjoyment • Many patients found it helpful if one individual took responsibility for organising their overall care and liaising with other health and social care professionals. Some patients had very involved GPs who took on this role, others hardly saw their GP. Some patients and their carers were very proactive in organising their own care package although this took a deal of time and energy. • Aims of the study • Explore patients’ experiences of communication between and within the various groups of health and social care professionals involved in the delivery and management of their care. • Identify the factors patients perceive to be influential in facilitating and inhibiting effective IIPC • Identify the impact that effective IIPC, or lack of it, has on patient defined outcomes in the palliative care setting. What are patients’ experiences of communication across the different professions and locations of care? Illustrative Quotes Example of Good IIPC “…I’m very fortunate in having a GP who I consider to be, well he’s very co-operative and knowledgeable and also has contact with the other two, with the two consultants. . . all three of them well whenever I have for example a meeting with [consultant] . . . copies of our meeting letters which contain information about our meeting, copies are sent to the oncology specialist, to my GP and also to myself.. . .. .he [GP] has sometimes phoned [consultant] …he opens his phone and he’ll let [consultant] know that my husband and I are with him and we have a three-way conversation on the phone. Patient 7 Example of IIPC problem 1 “…… they did another CT scan following my discharge, but I couldn't find out any information from it. I went to the oncologist . . .and he said he didn't know I'd had a scan, but of course it transpired that he had ordered it. Well quite frankly I didn't know what was going on. Anyway, I spoke to my own doctor again about it and he wrote or he phoned the hospital and he got a copy of the report and he sat down and read it out in front of me. . .It's not a question of finding out what's going on its finding out who will give me the information, this is my problem.. . basically I find that you've got so many people running round, you see at the moment I'm under the, still under the consultant for asthma problems and then I've got an oncologist, then I've got a cancer specialist nurse, then I've got a respiratory specialist nurse …I don't know whether they do [communicate together] or not because if they do they don't tell me.. . .I mean obviously each department has got access to my notes but… you know they never pass the information on…” Patient 10 Methods Data Collection. Twenty-two in-depth audio-tape recorded interviews were carried out. These were held in private where possible at a location convenient for the patient. Eighteen interviews took place in a side room/interview room within the palliative care centre. Three interviews were carried out in the patient’s home and one was carried out by the patients bed in an open ward. Interviews ranged in length from 15-60 minutes (mean 38 minutes.) Data Analysis. All interviews were transcribed fully and analysed with the assistance of Ethnograph a software package that aids the manipulation of textual data. Analyses were informed by some of the principles of Grounded Theory and carried out simultaneously with data collection. Interesting areas emerging from the analysis were followed up in subsequent interviews. Data collection ceased when no new information was emerging from the data Example of IIPC problem 2 “… I find it surprising that medical people don’t seem to communicate with each other ‘cause I had a bone scan a little while ago and I had occasion to visit {GP} I said do you know what the result is and he said they don’t tell me unless I ask. …..I thought you wouldn’t believe this would you cause I mean your GP is the pivotal bloke really he may not be the most expert but at least he’s at the command post. Patient 5 Patient as co-ordinator of care “....the consultant came in one day and I asked him. .. I told him I was ready to go home and he said “yes”, so I said “right if that's the way you're thinking and I'm glad that it is, could you get somebody to contact social services because at six o'clock the following morning I will have been in hospital for three weeks. … Now er I know you're saying “so what” and you might think so what but after the three week period social services and most agencies cancel the care package and you have to be reassessed from scratch. ….” Patient 20 Participants Following ethical approval and after informed consent 22 patients (11 each) from two specialist palliative care units agreed to participate in the study. Nine patients were male and 13 (59%) were female. The age range is 22-88 years old (Mean 65.9 years old, St Dev. 16.4). Time since initial diagnosis 8 weeks to 32 years (mean 4.86 years). Family member as co-ordinator of care “…. and the when the nurse came last Friday to change [patient’s] bandages I had left a message at the surgery that the doctor wanted to see so she had arranged to come and change them when the GP would be here……A big relief really cause she didn’t have to take them off again and put them back on again…’cause I just thought that you know they have so much to do that it might just, so I just asked the receptionist to write it in the nurses book and just jog their memory… Wife of patient 3 Referral to Specialist Palliative Care Service Primary diagnosis of patient participants • Time since referral to service • Range 1 week to 6 years • Average 1.2 years, St Dev. 1.73 Conclusions Problems associated with IIPC appear rare, but when they do occur they can cause patients and their family considerable anxiety and distress. Patients and their family carers are ideally placed in the centre of care events and so can facilitate communication across the different professionals and locations of care they are given. This does however place a burden upon the them at a time of difficulty. A great deal of IIPC is achieved out of sight from patients and carers, but more explicit pathways of communication would release patients and their family carers from unnecessarily spending time and energy monitoring and relaying information between different professionals and settings. References (1) Zwarenstein, M. and Bryant, W. (2001) Interventions to promote collaboration between nurses and doctors. The Cochrane Library (Oxford) 2001 issue1 online/ CD Rom (2) Hampson, J. P., Roberts, R. I., Morgan, D.A. (1996) Shared care: a review of the literature Family Practice 13/3 264-279. (3) Evans, D. (1996) A stakeholder analysis of development at the primary and secondary care interface. BritishJournal of General Practice. 46/412 675-677. (4) Beaudin, C. L., Lammers, J.C. and Pedroja, A. T. (1999) The role of organized communication: patient perceptions of efforts to coordinate hospital care. Abstract. Book. Assoc. Health Service Res. 16, 331 Ethical approval REC REF NO. 142/02l This project was funded by HOPE Innovation Fund