Download
1 / 24
280 likes | 919 Views
Congenital Hip Dislocation. Introduction. THA in the DDH patient presents a difficult challenge to the reconstructive hip surgeon. Introduction. Mild dysplastic hips (Crowe I and II) usually have adequate bone stock and can accept standard components . Crowe II. Crowe I. Introduction.

E N D
Congenital Hip Dislocation
Introduction • THA in the DDH patient presents a difficult challenge to the reconstructive hip surgeon
Introduction • Mild dysplastic hips (Crowe I and II) usually have adequate bone stock and can accept standard components Crowe II Crowe I
Introduction Crowe III Crowe IV
Introduction • Crowe III and IV dysplastic hips can be difficult to reconstruct and have the potential for more intra-operative and postoperative complications
Introduction • Surgical Options are Numerous: • ? High Hip Center • ? Controlled Protusio • ? Structural Grafting • ? Specialized Components (e.g. Custom) • ? Oblong Cups • ? Cementation and/or Cemented Cups • Each has potential problems
Study Aim • The aim of the current study is to present our midterm results after primary THA in DDH (Crowe III and IV) patients
Study Design • Between 1990 to 2000 twenty -nine (29) cementless primary THA were performed in 24 patients (Crowe III and IV DDH patients) • 17 Female and 7 Male • Five pts had staged bilateral THA
Study Design • Average pt age = 49.5 yrs • 48% were Crowe III • 52% were Crowe IV • Average Follow-up was 5.5 years
Technique • All surgeries were performed through a posterior approach • Acetabular Reaming routinely resulted in medial and superior placement of a standard cup.
Results • No structural allografts were utilized during acetabular preparation
Results • Average Cup Size = 51 mm Range (42mm to 66 mm) • Average Stem Size = 12.0 mm Range (9.0mm to 16.5 mm) • Average Head Size = 28 mm Range (22mm to 32 mm) ****Note that these are standard implant sizes
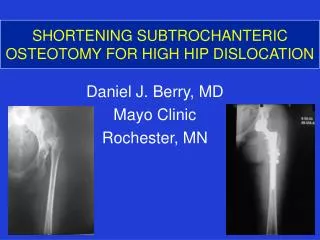
Results • 21% (6 pts) required a shortening osteotomy • All were type IV
Complications • Dislocations - 6.8% (2 pts) • (both eventually required conversion to a captured liner) • Aseptic Poly Wear - 13.8% (4 pts) • one required revision
Complications • Symptomatic H.O. - 3.4% (1 pt) • (Booker III, no surgery was required) • No Sciatic or Femoral Nerve complications
PM Pre
PM 14 days PM OR
PM Post 2 PM 18 mths
MC Pre MC Post MC 3yr
JG 5yrs. JG Pre
Conclusions • Crowe III and IV dysplastic hips can be routinely done without the use of structural allograft • Total Hip Arthroplasty (Crowe III/IVpts) can be routinely performed without the need for specialized components
Conclusions • Complications were low in this series • No Femoral or Sciatic Nerve Complications were observed • Dislocation rate of 6.8% • Only one poly exchange at 5.5 yrs
Conclusions • A Femoral Osteotomy is rarely required in Crowe III pts and only occasionally in Crowe IV pts • A Femoral Osteotomy was required in 6 Crowe IV pts (21%) No Crowe III pts required a femoral osteotomy (in this series)
Conclusions • Primary Total Hip Arthroplasty can be safely perfomed without the use of structural acetabular allograft in Crowe III/IV pts • Standard components can be utilized in a majority of cases and lesson the need for smaller “specialized” implants