Download
1 / 61
750 likes | 1.05k Views
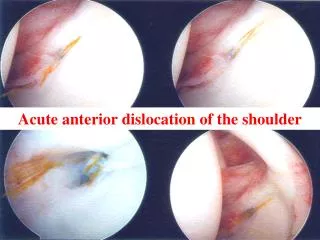
Shoulder Dislocation. s. Shoulder dislocation. 1. DISLOCATION - COMPLETE LOSS OF GLENOHUMERAL ARTICULATION . CAUSE- ACUTE TRAUMA 2 . SUBLUXATION - PARTIAL LOSS OF ARTICULATION WITH SYMPTOM’S. CAUSE- REPITITIVE TRAUMA.

E N D
Shoulder dislocation 1. DISLOCATION- COMPLETE LOSS OF GLENOHUMERAL ARTICULATION . CAUSE- ACUTE TRAUMA 2. SUBLUXATION - PARTIAL LOSS OF ARTICULATION WITH SYMPTOM’S. CAUSE- REPITITIVE TRAUMA. 3. LAXITY - PARTIAL LOSS OF GLENOHUMERAL ARTICULATION BUT PAITENT IS ASYMPTOMATIC. SHOULDER INSTABLITY
Shoulder dislocation • Shoulder is the most commonly dislocated joint[45%] 1] shallowness of glenoid socket 2]Extraordinary ROM 3] ligamentus laxity • Humeral head 3x larger than glenoidfossa • glenohumeral articulation is minimally constrained by bony anatomy alone • stability is conferred by a series of dynamic and static soft tissue restraints
Shoulder dislocation Type of dislocation Traumatic Dislocations Atraumatic dislocation Acquird dislocation
Traumatic dislocation Single force applies excessive overload to the soft tissues of the joint and often damages the Glenoid Labrum (Bankart Lesion) and the joint capsule Anterior [85%] Posterior[10] Inferior [5]
Atraumatic dislocation Athelete who has jointhyperlaxityand had multiple episode of joint subluxation Minor injury can results into dislocation [Congenital hypermobility or muscle weakness.]
Acquired dislocation • Sports such as swimming, gymnastics and baseball where repetitive micro-trauma, poor stretching and motion lead to capsular stretching. Eventual feeling of instability
Traumatic anterior dislocation Mech. of injury Arm in abduction and external rotation. Force is taken on the hand or arm which increases the external rotation of the arm causing the head of the humerus to dislocate
Clinical symptom: Pain [severe] Hold limb with normal limb by side of body. Abduction and external rotation. Pt can’t touch apposite shoulder [dugos test]
Clinical Evaluation • PE: • Prominent acromion, sulcus sign, palpable humeral head anteriorly • Neuro integrity of axillary and musculcutaneous nerves • Apprehension Test: reproduces sense of instability and pain in shoulder reduced prior to exam
Radiographic Evaluation • AP [fracture dislo] • Axillary • Special Views: • West Point axillary: for visualization of glenoid rim • Hill-Sach view: internal rotation view • Stryker Notch: view 90% of posterolateral humeral head
Management • Pre-Medication • Reduction Maneuvers • Post-Reduction Immobilization
Pre-Medication • Methods of Premedication prior to Reduction • None • Intraarticular Lidocaine • IV Sedation • Supraclavicular Block • Suprascapular Block
IV Sedation vs Intraarticular Lidocaine Injection Intra-articular Lidocaine Injection is Preferred over IV Sedation
Reduction Maneuvers • Is there an Ideal Method for Reduction? • Over 24 Techniques Described • Most Common Techniques • Kocher (71-100%) • External Rotation (78-90%) • Milch (70-89%) • Stimson (91-96%) • Traction/Countertraction • Scapular Manipulation (79-96%)
Kocher Maneuver TEA I • Traction • ER • Adduction • arm is internally rotated • Modified [no traction]
Traction/Countertraction • Arm in some abduction • Traction applied to arm • Assistant applies firm counter-traction with sheet across the body
Hippocratic method • Surgeon use foot applies on axilla for countertraction
Post-Reduction Immobilization • Is immobilization necessary? • What Method is Best?
Does immobilization reduce recurrence? • usually fracture associated with dislocation are reduced with reduction of dislocation. • Immobilization for 3-4 weeks after shoulder dislocation does NOT change the prognosis compared with immediate mobilization
Internal vs External Rotation • Level II RCT: Itoi JBJS 2007 • ER for 3 weeks • Recurrence rate: 32% • IR for 3 weeks • Recurrence rate: 60% • P = 0.007
Complication of ant.shoulder dislocation Early Rotator cuff tear Nerve injury Vascular injury Fracture dislocation
Late complication Stiffness Unreduced disloction [undiagnos in unconcious and old pts. ] closed reduction done upto 6 wks and open reduction done after 6wks in young pts. Willful neglect in old pts Recurrent dislocation
Post. Shoulder dislocation The arm is in flexion and adduction. Force is taken on the hand, causing the head of the humerus to be push out the glenoidposteriorly. h/o convulsion or electric shock
Clinical sign and symptom Diag is often missed Internal rotation Flat front of shoulder Prominent corocoid Frominent post aspect of shoulder
Radiology • AP- electric bulb apperence and empty glenoid sign. • Lat – post displacement
Treatmet Under GA reduction by pulling arm in adduction to dis engage head then lateraly rotate while pushing head anteriorly. Immobilization in ext rotation and abduction for 3 wks.
Inferior shoulder dislocation[luxatioerecta] Arm is in excessive abduction and a force is taken on the hand pushing the head of the humerus inferiorly out of the glenoid. Clinical features limb in abduction
Inferior shoulder dislocation[luxatioerecta] • Xrays –AP • LAT
Inferior shoulder dislocation[luxatioerecta] Treatment Traction and counter traction. Immobilised for 3 wks
Recurrent shoulder dislocation • Anterior dislocations account for ~95% of shoulder dislocations • Typically occurs in athletes who are < 25 years old • Males are much more commonly affected than are females (85-90%)
Recurrent shoulder dislocation • Pathology most commonly found in shoulders following a dislocation is a Bankart lesion • Disruption of the labrum and the contiguous anterior band of the inferior glenohumeralligamentous complex (IGHLC) • Bankhart lesion occurs > 85% of the time
Hillsach lesion – posteriolateral indentation of humeral head. • Enganging lesion is indication of surgery
Recurrent shoulder dislocation • Classification • Instability can be classified by: • direction of instability (anterior, posterior, multidirectional) • degree of instability (subluxation, dislocation) • etiology (traumatic, atraumatic, overuse) • timing (acute, recurrent, fixed)
Recurrent shoulder dislocation TUBS or “Torn Loose” • T raumatic aetiology, U nidirectional instability, B ankart lesion is the pathology, S urgery is required • AMBRI or “Born Loose” • A traumatic: minor trauma, M ultidirectional instability may be present, B ilateral: asymptomatic shoulder is also loose, R ehabilitation is the treatment of choice, I nferior capsular shift: surgery required if conservative measures fail
Recurrent shoulder dislocation Shoulder Stabilisers – Static Intracapsular pressure Labrum: increases depth of the glenoid by 50% Ligaments – main static restraints capsule
Shoulder Stabilisers Dynamic Rotator cuff and biceps