Download
1 / 33
390 likes | 818 Views
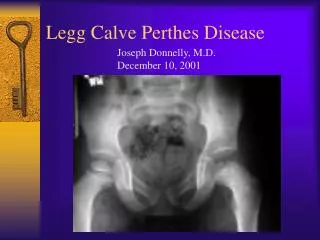
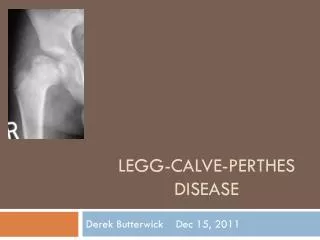
Surgical Treatment for Perthes Disease. Mazloumi MD Associated professor Orthopaedic surgeon. A 14-year-old boy who had Legg-Calve´- Perthes disease at age 8 years and was treated with nonoperative methods. Pathomechanical environment. Structural instability

E N D
Surgical Treatment for Perthes Disease Mazloumi MD Associated professor Orthopaedic surgeon
A 14-year-old boy who had Legg-Calve´-Perthes disease at age 8 years and was treated with nonoperative methods
Pathomechanical environment • Structural instability • Femoroacetabularimpingment • Articular incongruity (localized joint overload) • Abductor inefficiency (articular overload) • Combinations
Perthes deformities Proximal femur ( spectrom and variabilities of deformities) • Large and aspherical femoral head • High grater throchanter (over growth) • Short femoral neck • Head neck offset deformity • Varus neck- shaft angle • Osteochondral disease
Perthes deformities Acetabulom ( spectrom and variabilities of deformities) • Decreseadeanterolateral and/or posterolateral femoral head coverage. • Increased acetabular inclination. • Relative acetabular deficiency. • Variable acetabular version
Long term outcome of Legg-Calve-perthes at middle age • Risk of sever OA and clinically poor outcome after 40-50 years of age irrespective of prior successful surgical treatment and good outcome at skeletal maturity • Increased incidence of OA and THA in patients with a Stulberg class III / IV / V who were treated with conservative methods
Surgical approaches for treatment of sequelaeof Perthes disease • Extraarticular methods • Intertrochantericvalgusosteotomy • 1- Valgus extension: best corrects limb deformity • 2- Valgus flexion: may better correct anterior impingement • Trochanteric transfer with relative neck lengthening To correct greater trochanteric abutment) • Noncontainmentacetabular procedures • 1- Shelf acetabuloplasty • 2- Chiari procedure • Intraarticular methods • Osteochondroplasty of the head and neck (open or via arthroscopy) • Note: residual dysplasia may also require treatment • Femoral head reduction (central “downsizing”) Unproved method • Excision of osteochondritisdissecans • Labral repair
Femoral head reduction osteotomy (FHRO) technique ( Coxa magna )