Download
1 / 38
400 likes | 1.22k Views
Surgical Intervention for Carotid Artery Disease. Mr Gabriel Sayer Consultant Vascular Surgeon. Aims. Discuss the role Carotid Artery Stenosis (CAS) in the development of stroke Review different treatment modalities for CAS Appraise best practice guidelines

E N D
Surgical Intervention for Carotid Artery Disease Mr Gabriel Sayer Consultant Vascular Surgeon
Aims • Discuss the role Carotid Artery Stenosis (CAS) in the development of stroke • Review different treatment modalities for CAS • Appraise best practice guidelines • Identify how we can reduce strokes secondary to carotid artery stenosis in our patient population
Why is carotid artery stenosis important? • Risk factor for embolic stroke • Risk factor for ischaemic heart disease • Should therefore consider secondary prevention measures in all patients who have any carotid artery stenosis
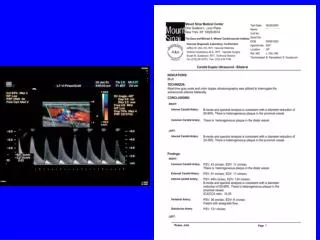
What is a carotid stenosis and how do we define it?? • Historical perspective • Clinical evaluation • Diagnostic modalities • Symptomatic ?
Carotid Artery Stenosis (CAS) and Stroke • Historically it was felt that CAS was associated with an increased risk of stroke • Diagnosis was difficult (combination of clinical and angiography) • Fischer M noted that often the carotid vessel distal to the stenosis was normal calibre
Carotid angiography But angiography had a procedural stroke risk of 0.1-1%
What is a symptomatic CAS? • ANY CAS associated with development of focal neurological episode in the area supplied by the corresponding middle cerebral artery or branches thereof
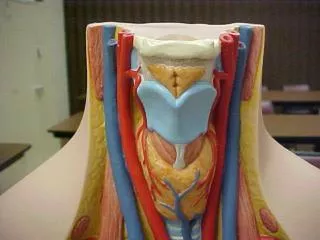
Carotid Artery Stenoses • Symptoms due to narrowing of the Internal Carotid Artery • The narrowing may be irregular promoting production of ‘emboli’ • Patients may suffer Amaurosis Fugax, TIAs or CVAs due to impaired blood supply to the brain
Treatment options • Ligation • Bypass • Endarterectomy
DeBakey- the greatest surgeon ever? • Worked under Leriche in Strasbourg and Kirschner in Heidelberg • Worked throughout europe during WWII culminating in the development of MASH units • First ever aortic aneurysm repair (1953) • First ever CEA (1953?) • First coronary artery bypass (1964) • First ventricular assist device (1966) • First multi organ transplant ….
The british version • 66 y.o female presented with recurrent bouts on LEFT monocular blindness and RIGHT hemiplegia • Professor Pickering organised a carotid angiogram • Professor Charles Rob supervised his Assistant director Felix Eastcott who undertook the operation
How do we do surgery for CAS? • Local or General anaesthetic? • Patch or not? • Shunt or not? • Eversion or open endarterctomy?
Results count, Method is secondary • GALA trial shows no benefit of LA over GA!
Carotid Endarterectomy- high risk patients • Challenging Anatomy • High carotid bifurcation • Distal disease • Redo operations • Previous surgery or RXT to neck or cranial nerve injury (esp RLN) • Crescendo TIAs • Medical comorbidity
What is evidence for treatment? • ESCT/NASCET • ACST
Level 1 Data in support of CEA as treatment for symptomatic CAS • Doubt over efficacy of the treatment and the advent of managed care led to two trials ECST and NASCET 1991 • Results are now 17 yrs old! • Selected population • Very little risk factor modification
NASCET Vs ECST • NASCET • 1-a/b x 100 = stenosis % • ECST • 1-a/c x 100 = stenosis % So ECST gives greater percentage of stenosis for same lesion
ECST/NASCET • Selective criteria for trial e.g. <80 years • NASCET approval required for surgeons • How applicable are these trials to real life
What about asymptomatics CAS? • Casanova 1991 • Veterans affairs study group 1993 • ACAS 1995 • And now the ACST 2005
ACST Summary • Significant reduction of stroke risk in asymptomatics CAS >70% with CEA • Procedural risk <3% major stroke or death • ACST • All stroke reduction of 6.4% versus 11.8% • 3.5% versus 6.1% for fatal or disabling strokes (net gain 2.5%) NNT=40
The End of Carotid Endarterectomy? • Now we can stent them • Is this better? • Is it suitable for all? • Does it last as long? • Should we do asymptomatics?
Potential advantages of carotid stenting • Reduced hospital stay • No wound complications • No cranial nerve injury vs 3-7% for CEA • Reduced cardiovascular complications
BUT.. • Is it durable? • Is there a higher procedural risk of stroke? • Up to 60% not suitable
Evidence • CAVATAS • LEICESTER • WALLSTENT • LEXINGTON Symptomatic and Asymptomatic • EVA-3S • SAPPHIRE • SPACE • ICSS (CAVATS II)
CAS Vs CEA • CEA is proven procedure • CAS has variable results although they appear to be improving with better kit and knowledge base • CAS probably has a 7-10% major stroke/death rate for symptomatic >70% • CAS not suitable for all
CEA vs CAS • The jury is still out and CAS remains the gold standard at present • ICSS trial will report soon and will shed further light on this area
When should we treat patients with intervention? • Within 6 months? • Within 2 weeks? • Within 2 days?
How we can reduce strokes secondary to carotid artery stenosis in our patient population ?