Download
1 / 35
350 likes | 448 Views
Multi-vessel disease and intracoronay physiology Combat MI 2009. Kees-joost Botman MD, PhD Catharina hospital Eindhoven Heart Institute The Netherlands. PCI vs CABG in multivessel disease: THE TAILORED APPROACH. background considerations (1):.

E N D
Multi-vessel disease and intracoronay physiologyCombat MI 2009 Kees-joost Botman MD, PhD Catharina hospital Eindhoven Heart Institute The Netherlands
PCI vs CABG in multivessel disease: THE TAILORED APPROACH background considerations (1): For years, cardiologists and cardiac surgeons have disputed about the optimum treatment of MVD : “ Is CABG the treatment of choice ?” “ Is PCI the treatment of choice ?” BUT......not all patients are the same !!
PCI vs CABG in multivessel disease ARTS – Study: IN MULTIVESSEL DISEASE: CABG and STENTING are equally effective treatments to prevent death and AMI, but excess repeated revascularization and more angina in STENT group The decision for revascularization of a particular lesion was based upon angiography ( stenosis > 50%)
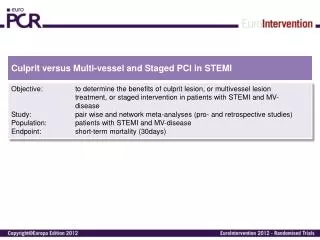
PCI vs CABG in multivessel disease SYNTAX – Study: IN MULTIVESSEL DISEASE: CABG and STENTING are equally effective treatments to prevent death and AMI, but excess repeated revascularization and more angina in STENT group The decision for revascularization of a particular lesion was based upon angiography ( stenosis > 50%)
PCI vs CABG in multivessel disease: THE TAILORED APPROACH background considerations (2) In patients with similar degree of anatomic disease, the most important predictor of outcome is the presence and extent of inducible ischemia(Beller,Circulation 2000): 12000 patients with MVD, similar severity of angiographic abnormalities: MIBI negative 0.6 % per year mortality / AMI MIBI positive 7.2% per year mortality / AMI
PCI vs CABG in multivessel disease: THE TAILORED APPROACH background considerations (3) AND : Revascularization is warranted for functionally significant stenoses only (DEFER study, Circulation, june 2001)
The DEFER Study: Adverse Events Death, AMI, CABG and (re)PTCA
PCI vs CABG in multivessel disease THE TAILORED APPROACH THEREFORE: Simply treatingall patients with multivessel disease in the same way ( either CABG or PCI ) makes little sense and is a rather crude approach TAILORED APPROACH Split up the multivessel population in two groups depending on the functional extent of disease, by assessing the functional significance of the individual stenoses
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: THE TAILORED APPROACH background considerations (4) In many patients with multivessel disease, non-invasive testing can not indicate which of several stenoses are culprit, but..... Fractional Flow Reserve (FFR), calculated from coronary pressure measurement, is an easy and accurate index to indicate specifically which lesions are culprit and which are not
Introduction • 24 def/spuit + draad
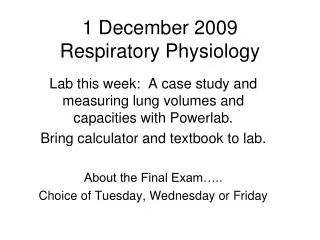
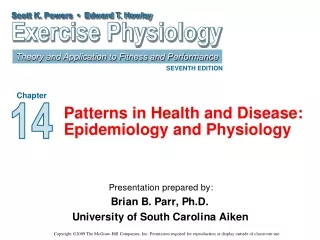
Aorta Krans slagader 100 0 Qnormaal 100 Pa=100 Perfusiedruk 100 mmHg 100 0 Pd=70 Pa=100 Qstenose ΔP 30 mmHg Perfusiedruk 70 mmHg Maximale hyperaemie Hartspier Qsten/Qnorm = Pd / Pa = 0.70 (70%)
1000 X 0.014 inch
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: THE TAILORED APPROACH • 150 patients with multivessel disease, • ARTS and SYNTAX like characteristics (410 stenoses) • Coronary Pressure measurement in all stenoses • If FFR < 0.75 stenosis considered as “culprit” • If FFR > 0.75 stenosis “non - culprit” If 3 culprit lesions or 2 culprit lesions including LMCA : CABG If 1 or 2 culprit lesion (not incl LMCA) : PCI Botman CJ et.al, JACC 2001
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: THE TAILORED APPROACH In this way, the population with multivessel disease was split up in two groups, not distinguishable by the degree of angiographic abnormalities, but with different degree of functional disease.
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: THE TAILORED APPROACH • 150 patients • 410 stenoses: FFR measured in 360 stenoses • total occlusion in 21 vessels: • culprit by definition • not able to measure: 7 stenoses • not “recognized” : 22 stenoses 259 culprit 101 not culprit
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: THE TAILORED APPROACH Based upon these measurements, 87 patients qualified for CABG and 63 patients qualified for PCI Risk factors and angiographic characteristics were completely similar in both groups 2 vessels: n=38 1 vessel: n=25
Angiographic characteristics of the culprit and non-culprit lesions
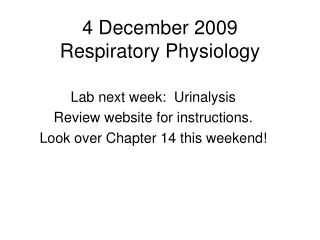
Male, 50-year-old Angina class 2-3 Positive ET
After stenting LAD
Optimum Revascularization Strategy for Multivessel Disease : THE TAILORED APPROACH Serruys, NEJM 2001; Botman, ESC 2002 Ww3139
SYNTAX Subgroup MACCE Rates at 12 Months CABG TAXUS* Patients (%) All LMN=705 LM IsolatedN=91 LM+1VDN=138 LM+2VDN=218 LM+3VD N=258 3VD ( w/o LM) N=1095 Comparisons for the LM and 3VD subgroups are observational only and hypothesis generating * TAXUSTM Express2TM Stent System Source: See Glossary
OPTIMUM TREATMENT OF MULTIVESSEL DISEASE: CONCLUSIONS: • In multivessel disease, coronary pressure measurement is an excellent tool to identify the culprit lesion(s) by • FFR < 0.75 • 2. In this way, patients with otherwise similar characteristics • can be stratified in 2 groups, according to the functional • extent of disease (“number of culprit lesions”): • PCI group: one or 2 culprit lesions; • CABG group: 3 or more culprit lesions) • PCI and CABG used in this way provide an equally effective treatment, both in terms of adverse events, repeated revascularization, and quality of life