Download
1 / 8
80 likes | 494 Views
PACCOCATH ISR. Treatment of In-Stent Restenosis by Paclitaxel Coated PTCA Balloons. Presented at The American Heart Association Scientific Session 2006 Presented by Dr. Bruno Scheller. PACCOCATH ISR: Background.

E N D
PACCOCATH ISR Treatment of In-Stent Restenosis by Paclitaxel Coated PTCA Balloons Presented at The American Heart Association Scientific Session 2006 Presented by Dr. Bruno Scheller
PACCOCATH ISR: Background • Treatment of coronary in-stent restenosis is hampered by high incidence of recurrent in-stent restenosis. • Multiple studies have shown the benefit of drug-eluting stents in preventing restenosis in de novo lesions, but only one randomized trial, ISAR-DESIRE, has been conducted for patients with pre-existing lesions. • While the ISAR-DESIRE trial showed a reduction in restenosis for drug-eluting stents compared with bare metal stents, the stent-in-stent approach for treating restenosis may not be optimal or feasible for all patients. • The goal of this trial was to assess the efficacy and safety of a paclitaxel eluting balloon catheter compared with a non-eluting balloon catheter among patients with coronary in-stent restenosis. Presented at AHA 2006
PACCOCATH ISR : Study Design 52 Patients with single in-stent restenosis in a coronary artery with a diameter stenosis of > 70%, < 25mm length, and vessel diameter of 2.5 mm to 3.5 mm; stable or unstable angina or a positive functional study. Randomized. Double-Blind. Parallel. 29% female, mean age 64 years, mean follow-up: 12 months Paclitaxel-Eluting Balloon Catheter (3 µg paclitaxel/mm2) n=26 Non-Eluting Balloon Catheter (same balloon design without drug) n=26 • Primary Endpoint: Angiographic late lumen loss at 6 months • Secondary Endpoint: Rates of restenosis; major adverse cardiac events (MACE) Presented at AHA 2006
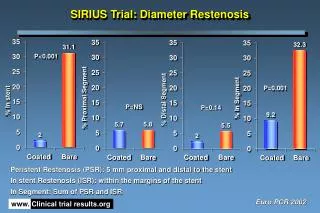
PACCOCATH ISR : Primary Endpoint In-segment late Lumen Loss (mm) • In-segment late lumen loss was smaller in the paclitaxel group than the bare balloon group (0.03+/- 0.48 vs. 0.74 +/- 0.86, p=0.002). • Minimum lumen diameter at 6-months was larger in the paclitaxel group than the bare balloon group (2.22 mm vs 1.57 mm, p=0.005). P=0.002 0.740 ± 0.86 mm 0.03 ± 0.48 Presented at AHA 2006
PACCOCATH ISR: Secondary Endpoint Binary Restenosis (%) p=0.002 • Binary restenosis occurred less frequently in the paclitaxel-eluting group than the bare balloon group (5% vs. 43%, p=0.002). Presented at AHA 2006
PACCOCATH ISR: Secondary Endpoint Rate of Major Adverse Cardiac Events (%) p=0.01 • At 12 months, the rate of major adverse cardiac events was 31% in the bare balloon group and 4% in the coated-balloon group (p=0.01). • This difference was primarily due to the need for target lesion revascularization in six patients in the bare balloon group (p=0.02). Presented at AHA 2006
PACCOCATH ISR: Limitations • The scale of the trial does not justify clinical application or regulatory approval of the drug-coated balloons. • Although the core laboratory was not aware of study-group status, the coated balloons have a faintly white color, a difference that might have unblinded the clinical investigators. • Larger clinical trials should be conducted in order to determine whether the results of this trial can be replicated. • This trial does not evaluate whether paclitaxel eluting balloons would be efficacious in the treatment of de novo lesions as opposed to in-stent restenosis. Presented at AHA 2006
PACCOCATH ISR: Summary • In this pilot study, treatment with a paclitaxel-eluting balloon catheter was associated with lower late lumen loss at 6 month angiography compared with a bare balloon catheter among patients with coronary in-stent restenosis. • The study also showed that treatment of coronary in-stent restenosis with paclitaxel-coated balloon catheters significantly lowered the incidence of adverse events. • The findings suggest that the inhibition of restenosis by local drug delivery may not require the implantation of stents and the prolonged release of a drug. Presented at AHA 2006