Download
1 / 86
920 likes | 1.27k Views
Diagnostic Imaging The Urinary System. Dr. LeeAnn Pack Diplomate ACVR. Retroperitoneal Space. Should be fat opacity ventral to sublumbar musculature Retroperitoneal fat allows visualization of the kidneys Thigh musculature often overlies caudal aspect and causes an increased opacity

E N D
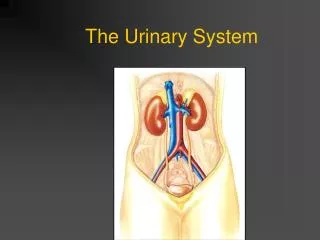
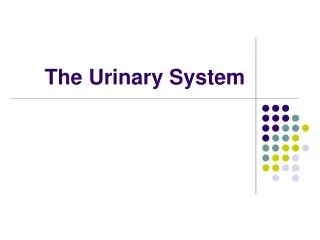
Diagnostic ImagingThe Urinary System Dr. LeeAnn Pack Diplomate ACVR
Retroperitoneal Space • Should be fat opacity ventral to sublumbar musculature • Retroperitoneal fat allows visualization of the kidneys • Thigh musculature often overlies caudal aspect and causes an increased opacity • Bifurcation of the deep circumflex iliacs often seen ventral to approximately L4
Retroperitoneal Space -Should be fat opacity -Thigh muscles will overlie caudal aspect
Retroperitoneal Space • Always examine the retroperitoneal space • Identify the kidneys cranially • Will see the sublumbar musculature • May see circular mineral looking opacities ventral to L4 and 5—circumflex iliac arteries • May see thigh musculature overlying the caudal aspect of the retroperitoneal space • Remainder should be fat opacity
Loss of Detail in the Retroperitoneal Space • Consider the following • Young animal with minimal body fat • Emaciated animal • Free fluid in the space • Mass in the space
Young Animal • This animal lacks body fat • Notice the poor detail in the retroperitoneal space and also in the peritoneal space
Fluid in the Retroperitoneal Space • Will see loss of detail • Fat opacity replaced with soft tissue-may have a streaky/whispy appearance • Most common fluids to consider are urine (generally trauma related) and blood (trauma, ruptured tumor, bleeding disorder • An IVP is indicated to distinguish
Fluid in the Retroperitoneal Space • Notice the loss of detail in the RS • Streaky soft tissue opacities are seen
Mass in the RPS • Will distend RPS if mass is large enough • May have mass effect on other organs • Consider kidney, adrenal, lymph node, body wall as most likely sources
Kidneys • Evaluate on both lateral and VD view • Best measured on the VD view • Right kidney—T13-L1 (dog), L1-L4 (cat) • Left kidney—L2-L4 (dog), L2-L5 (cat) • Dog: 2.5-3.5 times the length of L2 • Cat: 2.4-3.0 times the length of L2
Canine rt lt
Feline -kidneys usually easier to ID -shape is more round than the dog
IVP • Also called EU- excretory urogram • Start with a well prepared abdomen (enema) • Patient must be well hydrated! • Always do survey films • Inject 400mg I/lb intravenously as a bolus • Acquire films immediately, 5, 10, 20 and 40 minutes (both lateral and VD)
IVP Phases • Arteriogram-immediately • Nephrogram-within 20 seconds of injection • Pyelogram-begins 3-5 minutes post injection • Cystogram-as contrast is cleared into the lower urinary tract
Arteriogram • Documents initial blood flow to the kidney • Phase is very short • Seldom imaged • Occasionally will see a vascular blush if the first image is literally taken immediately at the time of injection
Nephrogram • Contrast is filtered and accumulates within the renal tubules • Should see good initial opacification that gradually fades over the study period • Opacification of the kidneys should be uniform and symmetrical
Pyelogram • Contrast is outlining the collecting system • Will be able to evaluate the renal pelvis and diverticuli • Pelvis should be <2mm wide • Recesses should be <1mm wide • Proximal ureters should be <2.5mm
Cystogram • This is contrast material entering the lower urinary tract • Will see segmental images of the ureters and the outline of the bladder • A formal cystogram is superior for imaging the bladder
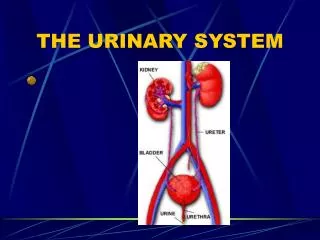
Renal Anatomy -renal pelvis -renal sinus -diverticuli -cortex -medulla -ureter
Normal IVP-Immediate Films Nephrogram Phase
Normal IVP-Five Minutes Nephrogram and Pyelogram
Normal IVP-Twenty Minutes Pyelogram and Cystogram
Contrast Induced Renal Failure • See opacification of kidneys that persists or becomes more intense over time • Hypotension—acute tubular necrosis—tubular obstruction—acute renal failure • Generally reversible but important to recognize this • Liver and GI are alternative routes of excretion
Contrast Induced Renal Failure-several hours post IVP -kidneys still opacified -contrast material within Gi tract -contrast material within the gall bladder
Kidneys • Always assess for number, size, shape, margination, location and opacity • Changes observed on radiographs will help you to refine your differential diagnosis list • Can you see them? Normal in size? What is the contour like? Any opacification changes?
Small Regularly Shaped Kidney • Most likely a congenital anomaly-hypoplasia • Usually bilateral and therefore usually young dogs with signs of renal disease • Can see with some chronic diseases but those are more commonly irregularly shaped • IVP-usually poor but uniform opacification with normal clearance into the lower urinary tract
Small Irregularly Shaped Kidney • May involve one or both kidneys • Consider the following • End-stage kidney • Infarcts • Chronic pyelonephritis • Chronic nephritis
Renal Irregularities Note the renal marginal irregularities
Large Regularly Shaped Kidneys • May be unilateral or bilateral • Consider the following • Acute pyelonephritis/nephritis • Hydronephrosis • LSA • Large parenchymal cyst or perirenal pseudocyst • FIP • Amyloidosis • Compensatory hypertrophy
Hydronephrosis-Bilateral -Suggestive of obstruction at trigone -This was secondary to TCC
Hydronephrosis-Unilateral -Hydronephrosis secondary to TCC
Polycystic Renal Disease • Most commonly diagnosed in young Persians and Himalayans • Congenital disease-multiple parenchymal renal cysts • May have cysts in other organs -liver, pancreas
Polycystic Renal Disease -Large irregularly shaped kidneys -Cat is also in thin body condition-possibly secondary to renal dysfunction -Cysts enlarge and destroy normal tissue
Perirenal Pseudocysts • These are outside the renal parenchyma and may be within the capsule or outside the capsule • Most common in older male cats • Kidney is enlarged and smoothly marginated-shape depends on the symmetry of the cyst
Renal Neoplasms • Kidney(s) are generally enlarged and irregularly shaped due to a mass • Occasionally will see mineralization associated with the neoplasm • Nephrogram-inhomogenous opacification, marginal irregularity +/- filling defects • Pyelogram-pelvis and diverticuli may be distorted-mass could obstruct pelvis
Renal Neoplasm IVP-irregular margin -pelvic distortion Irregular on surveys
LSA • This is the most common renal neoplasm in the cat and also occurs in dogs • Generally bilateral • May be regular or irregularly marginated-some are more uniformly infiltrated • May see evidence of other organ involvement-spleen, liver, LN
Abnormal Renal Opacity • Mineralization-calculi, parenchymal mineralization or deposition, or neoplastic mineralization • Gas-may be renal or perirenal
Ureters • Small soft tissue structures extending from the renal pelvis to the bladder • Normally not seen on survey films
Hydroureter • Seldom seen on survey films • May see tubular soft tissue structure in the RPS if the dilation is severe • Best documented with contrast-IVP
Hydroureter -occasionally you may see enlarged ureters on plain films
Hydroureter -usually requires contrast opacification to identify the dilated ureter(s)
Ureteral Calculi • Examine the RPS carefully for mineral opacities • They may be very small-best seen on the lateral but try to identify on both views • *remember the deep circumflex arteries-they will look like small calculi
Ectopic Ureter • Usually shows evidence if hydroureter on that affected side • May also see hydronephrosis in the kidney • Ureter may enter the vagina, tunnel by bladder, urethra etc. • Oblique views made at 5 minutes
Ureteral Rupture • Most of the ureter is within the RPS—becomes peritoneal as it enters the bladder • May see loss of detail in the RPS or the peritoneal space due to urine leakage • IVP-free contrast material in the RPS or the peritoneal space