Download
1 / 30
300 likes | 602 Views
Sleep What is normal?. Dr Andrew Mayers amayers@bournemouth.ac.uk. Sleep. Overview Normal sleep How much should we get? Sleep disorders Insomnia and hypersomnia Narcolepsy Sleep Apnoea Circadian rhythm disorders Poor sleep and depression. An overview of normal sleep.

E N D
SleepWhat is normal? Dr Andrew Mayers amayers@bournemouth.ac.uk
Sleep • Overview • Normal sleep • How much should we get? • Sleep disorders • Insomnia and hypersomnia • Narcolepsy • Sleep Apnoea • Circadian rhythm disorders • Poor sleep and depression
An overview of normal sleep • What is normal sleep? • Average sleep 6½ - 8 hours each night • Regulated by 25-hour circadian rhythm • Adjusted to coincide with normal wake-sleep routines • Use cues from environment • Clocks and sunlight/darkness (Thase, 1998) • Much of what we learn here can be read in my review (Mayers & Baldwin, 2006) • But, before we see what is measured… • We should understand how sleep is measured
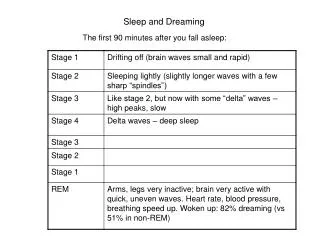
Normal sleep • Sleep EEG stages (Rechtschaffen and Kales, 1968) • Stage 1 – light sleep • Similar to alert wakefulness • 2-5% of ‘healthy’ sleep episode • Stage 2 – getting deeper… • About 55% of sleep episode • Stages 3 and 4 usually examined together • Often referred to as slow-wave sleep (SWS) • About 13-25% of sleep episode
Normal sleep • Sleep EEG stages • Sleep usually divided into 4 to 6 cyclic progressions • SWS • Predominates in early sleep episode • Rapid-eye-movement (REM) sleep • Appears after 1st cycle • Periods of intense brain activity • Frequent and intense bursts of eye movement • But with lack of muscle tone elsewhere • First REM period usually occurs after 60-110 minutes • REM sleep periods get longer and denser across night
REM sleep vs. SWS • SWS associated with human growth hormone (GH) • If SWS reduced, then so is GH(Van Cauter & Copinschi, 1999) • Low GH may be associated poor quality of life • SWS probably associated physical restoration • REM sleep commonly associated with dreaming • Dreams can often reflect current thinking styles and mood • REM sleep often seen as psychological ‘filing system’ • Depression associated with REM/SWS disruption • SWS REM (Benca, 2001) • Most antidepressants suppress REM sleep • We will discuss this later
Sleep: where does it go wrong? • We will now look at examples of sleep disorders • Not enough time to review them all • But we will explore some of most common ones • Many of the sleep disorders relate to sleep stage disruption • While others relate to unusual occurrences during sleep • Sleep disorders categorised according to nature • Dyssomnias • Sleep timing, stage disruption and sleep quality • Parasomnias • Physical and behavioural abnormalities during sleep • We will not look at that today (but do ask if you want to know more)
Insomnia • Most common sleep disorder • Problems initiating sleep (early insomnia) • Maintaining sleep (middle insomnia) • Or early morning awakening (late insomnia) • At least 2 weeks (nearly every day) for 1 month or more • Phillippa will look at this in more depth later • Can lead to significant problems • Physical health • Impairment in normal functioning… • Chris will explore this • Mental health – especially depression • I will discuss this further
Narcolepsy • Features (Overeem, et al. 2001) • Excessive daytime sleepiness (EDS) • May be as mild as subjective feelings of sleepiness • Or as extreme as sudden irresistible sleep attacks • Hypnagogic hallucinations • Often frightening images that occur at sleep onset • Usually visual, but can be auditory • Cataplexy • Sudden collapsing and total muscle tone loss • Most often in association with intense emotion • Usually laughter or excitement • Sleep paralysis • Narcoleptics go straight into REM sleep
Sleep apnoea • Obstructive sleep apnoea (OSA) • Patients briefly stop breathing during sleep • Similar to choking • Causes brief arousals • Followed by ‘snoring’ • Patient (normally) returns to normal breathing • Little physical damage as a result • Central sleep apnoea (CSA) • More rare, but potentially more damaging • Breathing stops for long periods • May even cause death
Sleep apnoea • Consequences • Sleep disruption • Poor concentration, car accidents, etc • High blood pressure • Breathing stops frequently during the night • Increased stress on the heart • Heart has to work harder • Increases blood pressure • Among OSA pts without high blood pressure • 45% will develop this within 4 years • Among patients with the highest blood pressure • 80% have OSA
Circadian rhythm sleep disorders (CRSD) • Misalignment of patient’s sleep patterns and ‘societal norm’ • Sleep occurs at wrong time of day • Or ‘out of phase’ • CRSD sleep disorders: • Jet lag • Shift work • Sleep phase syndromes • CRSD associated with other circadian rhythm-related factors • Melatonin release and body temperature (Dagan, 2002)
Relationship between insomnia and depression • One-third of patients with chronic sleep problems present mood disorders • Most patients with mood disorders experience insomnia • And, less often, hypersomnia (Benca, et al. 1997) • Poor sleep implicated in most psychiatric disorders • But more pervasive and consistent in depression • Sleep disturbance common in suicidal patients • Subjective sleep quality poorer in suicidal depressed pts (Singareddy & Balon, 2001)
Insomnia and depression • Sleep EEG analyses (Benca, et al. 1997) • Depressed patients show: • Shorter total sleep time • Longer sleep latency • Less slow-wave sleep • Shorter REM latency • Greater REM density • Compared to controls
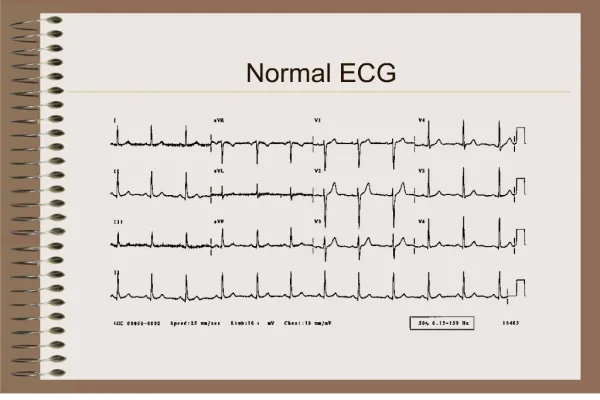
Sleep EEG • Sleep EEG in healthy person Sleep EEG in depressed pt
Insomnia may predict depression • Longitudinal study (Ford and Kamerow, 1989) • Insomnia and depression measured at baseline/1 year follow up • If insomnia present at both time points • Risk of developing depression 40x greater • Than if no insomnia present • If insomnia resolved by follow up • Risk of developing depression 2x greater • Another seminal study (Breslau et al. 1996) • Similar to Ford & Kamerow, but 3.5 year follow-up • If history insomnia at baseline • Risk of developing first depression by follow-up 15.9% • No history of insomnia at baseline, risk = 4.6% • 4x more likely to develop ‘new’ depression • 3x more likely with history hypersomnia
Sleep perceptions in insomnia and depression • Differences in sleep perception between insomnia and depression • Longitudinal studies focus on diagnoses • Also tend to use objective measures – sleep EEG • But sleep perceptions also important • These may differ between insomnia and depression • Insomnia may be related to anxiety • Cognitive bias focus on perceptions of sleep timing (Harvey 2000, 2002, 2003) • Depression related to perceptions of sleep satisfaction (Mayers, et al., 2003; Mayers & Baldwin, 2006)
Insomnia and anxiety • Faulty sleep cognition implicated in insomnia (Harvey 2002, 2003) • Worry about poor sleep may maintain insomnia • Pre-sleep cognitive activity associated negative thoughts • Intensifies worry, especially about getting to sleep • Catastrophisethe impact (Harvey 2003) • Daytime function • Work performance • Social relationships • This serves to exacerbate the sleep problem • Self-fulfilling prophecy
Sleep perceptions and depression • Sleep cognitions also implicated in depression • But tend to reflect negative thoughts (Beck 1987) • Negativity may explain sleep perception inaccuracy in depression (Argyropoulos 2003) • We will see more about that shortly • Additional REM activity may be partial explanation (Johnson 2005) • Particularly as result of dreaming • Reduced rationality • Negative content and emotion • Sleep satisfaction may be more relevant in depression
Sleep perceptions and depression • Subjective sleep satisfaction measured in depressed populations • In one study • Depressed pts reported sig poorer satisfaction than controls • Even though sleep timing perceptions were similar between groups (Mayers, et al 2003) • In a later study • Variance in sleep timing perceptions was more likely to be explained by anxiety • And sleep satisfaction perceptions were more likely to be explained by depression (Mayers, et al 2009)
Effect of antidepressants on sleep • Antidepressants may help mood… • But they may also have an effect on sleep • The clinician must consider this when treating • In a review byMayers & Baldwin (2005) effects were examined across all types of antidepressant • Tricyclics (TCAs): e.g. amitriptyline • Often associated with sedation • Selective Serotonin Reuptake Inhibitors (SSRIs): e.g. Prozac • Frequently linked to insomnia • BUT supress REM sleep (more so than TCAs) • Useful for narcolepsy • Some newer meds (e.g. mirtazapine) similar to TCAs
Sleep disorders and depression • Narcolepsy • Several studies indicate relationship with mental well being • Narcoleptic pts demonstrated several problems: • Sig poorer quality of life perceptions vs. controls • Narcoleptic pts more likely to have mental illness (OR: 4.06) • Including depression • EDS may explain depression in narcolepsy – sheer fatigue • Narcolepsy associated with REM sleep abnormalities • Cataplexy often treated with antidepressants: • Suppress REM sleep … improve mood • Reduces cataplexy, sleep paralysis and hypnagogic hallucinations
Sleep disorders and depression • Obstructive sleep apnoea (OSA; Andrews & Oei 2004) • Several studies indicate relationship with mental well being • OSA pts showed more evidence of dep than controls • Depression in OSA may be secondary • Effect disappears when controlling for other factors • OSA associated with frequent arousals from sleep • This has impact on EDS leads to depression? • OSA associated with increases in Stage 1 sleep • Usually at the expense of SWS • Pt may not feel refreshed upon waking • So depression may be related to sleep satisfaction
Sleep disorders and depression • Circadian rhythm sleep disorders (CRSD) • CRSD may be associated with EDS • Which may be related to poor mood • But also linked with melatonin • Melatonin levels reduced in depression (Brown, 1985) • Depletion also observed in CRSD (Shibui et al 1999) • We will now see how this relates to CRSD types • Jet lag, shift work and delayed sleep phase syndromes
Jet lag and depression • Melatonin may be involved in triggering sleep • Via complex relationship with serotonin • We know that serotonin is strongly linked with depression (Idzikowski 1991) • Jet lag is linked with melatonin reduction • Jet lag associated with: • Fatigue, sleep schedule disturbance, impaired cognitive functions, and depression • More so with east-bound flights • Over 5 or more time zones • However, more likely to be related to relapse • Than new depression • Jet lag may exacerbate, rather than cause, depression (Katz et al 2002)
Shift work and depression • Regular shift workers appear to be more prone to depression • Shift workers present several problems (Sasaki & Takahashi 1990): • Insomnia, autonomic dysfunction, physical complaints, and depression • Shift workers show more problems than day workers (Drake et al 2004): • EDS, insomnia, absenteeism, accidents and depression • Females sig more prone to these effects than males • Depression (measured by BDI) worse for shift workers • Than traditional workers (Goodrich & Weaver 1998)
Sleep phase syndromes and depression • Advanced sleep phase syndrome (ASPS) is typical in older people • Earlier to bed; early morning awakening • Delayed sleep phase syndrome (DSPS) is typical in younger people • Later sleep onset times; late morning waking • ASPS has been associated with depression (Schrader et al 1996) • But DSPS receives most attention in the literature (Regestein & Monk 1995) • Three-quarters of DSPS pts had history of depression • For 50% of these, depression is resistant to treatment
Summary • Relationship between sleep disorders and MI mixed • Considerable evidence with insomnia and hypersomnia • Poorer sleep length and disturbance • Problems relating to sleep architecture • REM sleep vs. SWS • Although insomnia may be more related to anxiety • Particularly in respect of reports of sleep timing • Depression more likely to be related to sleep satisfaction • Antidepressants have marked effect on sleep • Whether positive or negative depends on type
Summary • Strong links between narcolepsy and depression • Particularly through EDS and cataplexy • Treatments for narcolepsy often relieve depression • Relationship with sleep apnoea less clear • Depression in OSA may be secondary • Although sleep satisfaction may be poorer in OSA • Depression found in other dyssomnias • Circadian rhythm disorders, jet lag, etc.