Download
1 / 53
530 likes | 788 Views
Advances in the Medical Management of Peripheral Arterial Disease. Randall M. Zusman, MD Associate Professor of Medicine Harvard Medical School Director Division of Hypertension and Vascular Medicine Massachusetts General Hospital Boston, Massachusetts. ?. Key Question.

E N D
Advances in theMedical Management of Peripheral Arterial Disease Randall M. Zusman, MD Associate Professor of Medicine Harvard Medical School Director Division of Hypertension and Vascular Medicine Massachusetts General Hospital Boston, Massachusetts
? Key Question How many of your patients with CV risk do you test for peripheral arterial disease? • 0%-24% • 25%-50% • 51%-75% • 76%-100% Use your keypad to vote now!
Faculty Disclosure • Dr Zusman:advisory board member, research support, speakers bureau: AstraZeneca,Bristol-Myers Squibb Company, Forest Pharmaceuticals, Inc., Novartis Pharmaceuticals Corporation, Pfizer Inc, sanofi-aventis Group, Sankyo Co., Ltd.
Learning Objectives • Describe the prevalence and disease burden of PAD • State medical treatments for improving leg symptoms of the patient with PAD • Discuss interventions used to prevent systemic complications in the patient with PAD PAD = peripheral arterial disease.
? Key Question How common is PAD? • 1-4 million Americans • 4-8 million Americans • 8-12 million Americans • 12-16 million Americans Use your keypad to vote now!
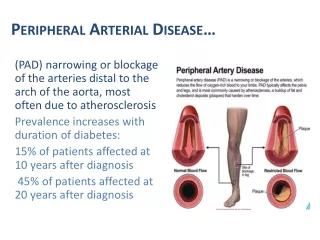
PAD: Scope of the Problem • PAD is caused by atherosclerotic occlusion of the arteries to the legs • Common, but often overlooked • Exact prevalence is unknown • PAD may be asymptomatic or present with atypical symptoms • Approximately 8-12 million Americans have PAD • Associated with significant morbidity and mortality resulting from MI, stroke, death MI = myocardial infarction. American Heart Association. Heart Disease and Stroke Statistics—2005 Update. 2005; Hiatt WR. N Engl J Med. 2001;344:1608-1621.
PAD: Scope of the Problem 16 PAD affects 8-12 million Americans, second only to CHD* Proportionately, for every 4 patients seen with CHD*, clinicians might expect to see approximately 3 patients with PAD 14 13 12 8-12 10 Prevalence (millions) 8 6 4 5.4 2 0 Stroke PAD CHD* *Includes MI and angina pectoris. CHD = coronary heart disease. American Heart Association. Heart Disease and Stroke Statistics—2005 Update. 2005.
PAD: Prevalence Increases With Age Rotterdam Study (ABI <.9) San Diego Study (PAD by noninvasive tests) 60 50 40 Patients With PAD (%) 30 20 10 0 55-59 60-64 65-69 70-74 75-79 80-84 85-89 Age Group (y) ABI = ankle-brachial index. Creager M, ed. Management of Peripheral Arterial Disease. Medical, Surgical and Interventional Aspects. 2000.
REACH—Scope of the Problem:Cerebro- and Cardiovascular Disease 63% of PAD patients had polyvascular* disease N = 7013 Cerebro-vascular Coronary artery 14.2% 9.5% 39.4% Peripheral artery Polyvascular disease *PAD patients with polyvascular disease had concomitant symptomatic cerebrovascular disease and/or CVD. REACH = REduction of Atherothrombosis for Continued Health. Bhatt DL et al. American College of Cardiology Scientific Session. March 8, 2005.
? Key Question PAD increases the risk of CHD death by approximately: • 1×-2× • 3×-4× • 5×-6× • 6×-7× • 7×-8× Use your keypad to vote now!
PAD: Increased Risk of Mortality Patients with large-vessel PAD* are at ~6×the risk of dying from CHD compared with patients without PAD 10.0 8.0 6.6 (2.9-14.9) 6.0 Relative Risk of Death (95% CI) 4.0 3.1 (1.9-4.9) 2.0 0.0 Death From Coronary Heart Disease All-Cause Mortality Cause of Death *ABI ≤0.8. Adapted from Criqui MH et al. N Engl J Med. 1992;326:381-386.
HOPEPAD: Increased Risk of Mortality PAD doubled mortality rate (17.5% vs 8.5%) after mean follow-up of 4.5 years Clinical PAD SubPAD ABI <0.6 SubPAD ABI 0.6- 0.9 No-PAD & ABI >0.9 0.25 0.20 0.15 Kaplan-Meier Rates 0.10 0.05 P <.0001 0 0 500 1000 1500 2000 Days of Follow-up HOPE = Heart Outcomes Prevention Evaluation. Ostergren J et al. Eur Heart J. 2004;25:17-24.
PAD in Primary Care: Underdiagnosed • Prevalence is high, yet clinician awareness of PAD diagnosis is relatively low • Simple ABI measurement identifies many patients with previously unrecognized PAD • Atherosclerosis risk factors are prevalent in patients with PAD • Received less intensive treatment for lipid disorders and hypertension • Prescribed antiplatelet therapy less frequently than patients with CVD Hirsch AT et al. JAMA. 2001;286:1317-1324.
PAD: Prevalence in the Primary Care Office Setting NHANES1 Age >40 4.3% The prevalence of PAD in primarycare clinics was almostin high-risk patients San Diego2Mean age = 66 11.7% 30% NHANES1Age ≥70 14.5% Rotterdam4Age >55 19.1% Diehm3Age ≥65 19.8% PARTNERS5 Age >70, or between 50-69 with history of diabetes or smoking 29% 0% 5% 10% 15% 20% 25% 30% 35% NHANES = National Health and Nutrition Examination Survey. PARTNERS = PAD Awareness, Risk, and Treatment New Resources for Survival program. 1. Selvin E, Erlinger TP. NHANES. Circulation. 2004;110:738-743; 2. Criqui MH et al. Circulation. 1985;71:510-515; 3. Meijer WT et al. Arterioscler Thromb Vasc Biol. 1998;18:185-192; 4. Diehm C et al. Atherosclerosis. 2004;172:95-105; 5. Hirsch AT et al. JAMA. 2001;286:1317-1324.
PARTNERSDetecting PAD With Symptoms The authors concluded that up to 90%* of patients with PAD would be missed if healthcare providers relied solely on the classic symptoms of intermittent claudication Healthcare providers should also routinely inquire about atypical symptoms 90% did not have classic intermittent claudication symptoms *In patients with ABI ≤0.9. Hirsch AT et al. JAMA. 2001;286:1317-1324
Typical Symptoms(Intermittent Claudication) ~10% • Exercise calf pain • Not present at rest • Relieved within 10minutes by rest Atypical Symptoms~50% Occlusion may develop slowly, allowing collateral circulation to develop PAD: Symptoms Patients With PAD Asymptomatic PAD ~40% Symptomatic PAD American Heart Association. Heart Disease and Stroke Statistics—2005 Update. 2005; Criqui MH et al. Vasc Med. 1996;1:65-71.
ABI Available ABI Not Available PAD: Diagnostic Critical Pathway Clinical Evaluation: History and Physical • Caveats for Referral toVascular Lab • Assessment of location/ severity is desired • Patients with poorly compressible vessels • Normal ABI where PAD suspicion is high • Vascular Lab Evaluation • Segmental pressures • Pulse volume recordings • Treadmill PAD Diagnosis PAD Diagnosis Adapted from American Diabetes Association. Diabetes Care. 2003:26;3333-3341.
? Key Question The most common risk factor for PAD is: • Diabetes • Smoking • Hypertension • Total cholesterol level Use your keypad to vote now!
PAD: Common Risk Factors* ◄Lesser risk Greater risk ► Diabetes 4.05 Smoking 2.55 Patients with diabetes are at a 4x higher risk of developing symptomatic PAD versus the general population Hypertension 1.51 Total cholesterol (10 mg/dL) 1.10 0 1 2 3 4 5 6 • Age >40 years *PAD diagnosis based on ABI <0.90. Newman AB et al. Circulation. 1993;88:837-845.
PAD: Physical Examination Additional examination by palpation and auscultation to detect abnormal aortic aneurysm or bruit Gey DC et al. Am Fam Physician. 2004;69:525-532.
Concept of ABI Systolic BP in the leg should be approximately the same as that in the arm Leg Pressure Therefore, the ratio of systolic BP in the leg versus the arm should be approximately 1 or slightly higher ÷≈ 1 Arm Pressure ABI is 95% sensitive and 99% specific for angiographically diagnosed PAD Adapted from Weitz JI et al. Circulation. 1996;94:3026-3049.
Measuring ABI • Gather equipment needed • Position patient • Measure the brachial BP • Position the cuff above the ankle • Measure pressure in the DP artery • Measure pressure in the PT artery • Repeat the process in opposite leg DP = dorsalis pedis; PT = posterior tibial. American Diabetes Association. Diabetes Care. 2003;26:3333-3341; Dormandy JA et al. J Vasc Surg. 2000;31:S1-S296.
Calculating ABI Right Leg ABI Left Leg ABI Higher right ankle pressure(DP or PT pulse) Higher arm pressure (either arm) Higher left ankle pressure(DP or PT pulse) Higher arm pressure (either arm) = = ABI Interpretation ≤0.90 is diagnostic of PAD Hiatt WR. N Engl J Med. 2001;344:1608-1621.
ABI Workshops • Demonstrations available throughout the day
358% 300% Weekly Increase in ABI Use in Office Monthly Increase in ABI Use in Office PARTNERSIncorporating ABI Into Primary Care After Clinicians Participated in PARTNERS: 88% Clinicians thought it feasible to incorporate ABI into daily practice Mohler, ER et al. Vasc Med. 2004; 9:253-260.
ABI Available ABI Not Available PAD: Diagnostic Critical Pathway Clinical Evaluation: History and Physical • Caveats for Referral toVascular Lab • Assessment of location/ severity is desired • Patients with poorly compressible vessels • Normal ABI where PAD suspicion is high • Vascular Lab Evaluation • Segmental pressures • Pulse volume recordings • Treadmill PAD Diagnosis PAD Diagnosis Adapted from American Diabetes Association. Diabetes Care. 2003;26:3333-3341.
Vascular Laboratory Results: Segmental Pressures • Segmental pressures can help localize lesion • Considered abnormal when there is a • >20 mm Hg difference between adjacent segments within the same leg and between the original segment and the corresponding segment on the contralateral leg Brachial Brachial artery Upper thigh Proximal femoral artery Lower thigh Distal femoral artery Calf DP, PT, and proximal arteries Ankle PT or DP artery Holland T. Ostomy Wound Manage. 2002;48:38-40,43-46,48-49.
Vascular Laboratory Test: Pulse Volume Recordings Provides Segmental Waveform Analysis, A Qualitative Assessment of Blood Flow UpperThigh LowerThigh Calf Ankle Normal Normal tracingincludes initial systolic peak with a dicrotic wave on the down slope PAD Abnormal tracingcharacterized by a rounded systolic peak that is lower, as well as the lack of a dicrotic wave on the downslope Data provided by Mark Creager, MD. Holland T. Ostomy Wound Manage. 2002;48:38-40,43-46,48-49.
Treadmill Test: Function Testing to Aid Diagnosis Clinical Evaluation: History and Physical Suspect PAD Atypical Symptoms for PAD ABI Normal ABI with typical symptoms of claudication • Treadmill Function Testing • Patients with claudication will normally display a drop in ankle pressure after exercise • May also be used to assess treatment efficacy and evaluate overall physical function PAD Diagnosis Adapted from American Diabetes Association. Diabetes Care. 2003;26:3333-3341.
? Key Question The goals of therapy for PAD are: • Relieve exertional symptoms • Improve walking capability • Improve quality of life • Relieve ischemic pain at rest • Heal ischemic ulceration • Prevent limb loss • All of the above Use your keypad to vote now!
PAD: Treatment Goals • For patients with claudication • Relieve exertional symptoms • Improve walking capability • Improve quality of life • For patients with critical leg ischemia • Same as above, and • Relieve ischemic pain at rest • Heal ischemic ulceration • Prevent limb loss Hiatt WR. N Engl J Med. 2001;344:1608-1621.
PAD: Aggressive Risk Factor Modification Essential—1 NRT = nicotine replacement therapy. Gey DC et al. Am Fam Physician. 2004;69:525-532; Hiatt WR. N Engl J Med. 2001;344:1608-1621; Stewart KJ et al. N Engl J Med. 2002;347:1941-1951.
PAD: Aggressive Risk Factor Modification Essential—Smoking Cessation 40 35 PlaceboNicotine replacement Buproprion Bupropion andnicotine replacement 30 25 Percentage of Patients Abstaining 20 15 10 5 0 6 months 12 months Jorenby DE et al. N Engl J Med. 1999;340:685-691.
179% 122% Percentage Increase Distance to Maximal Claudication Pain Distance to Onset of Claudication Pain At 6 months Meta-AnalysisSupervised Exercise Essential to Improve Intermittent Claudication Symptoms AMA has published a CPT code for supervised PAD rehabilitation (93668)2 • Greatest improvement: • Sessions lasted >30 min • 3 sessions/wk • Walk to near-maximal pain • >6-month program CPT = current procedural terminology. 1. Gardner AW et al. JAMA. 1995;274:975-980; 2. Kanjwal MK et al. JK–Practitioner. 2004;11:225-232.
PAD: Aggressive Risk Factor Modification Essential—2 A1C = glycosylated hemoglobin.Gey DC et al. Am Fam Physician. 2004;69:525-532; Hiatt WR. N Engl J Med. 2001;344:1608-1621; Norgren L et al. J Vasc Surg. 2007;45:S5A-S67.
HPS PAD: Aggressive Risk Factor Modification Essential—Lipids 0.4 0.6 0.8 1.0 1.2 1.4 Simvastatin Better Placebo Better HPS = Heart Protection Study. HPS Collaborative Group. MRC/BHF. Lancet. 2002;360:1329-1239.
HOPE PAD: Aggressive Risk Factor Modification Essential—Antihypertensive Therapy 0.6 0.8 1.0 1.2 Relative Risk in Ramipril Group HOPE Study Investigators. N Engl J Med. 2000;342:145-153.
PAD: Antiplatelet and Vasodilator Therapy ACCP = American College of Chest Physicians; ASA = aspirin; CAPRIE = Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events;CCB = calcium channel blocker; CHF = chronic heart failure; GI = gastrointestinal; TTP = thrombotic thrombocytopenic purpura. Adapted from Gey DC et al. Am Fam Physician. 2004;69:525-532.
CAPRIEClopidogrel Versus ASA: MI, Ischemic Stroke, or Vascular Death 16 8.7% Overall RRR (P = .045)* Clopidogrel ASA 5.83% 12 5.32% (N = 19,185) 8 Cumulative Event Rate (%) Subjects had a recent MI, recent ischemic stroke, or symptomatic PAD 4 0 0 3 6 9 12 15 18 21 24 27 30 33 36 Months of Follow-up Median follow-up = 1.91 years *ITT analysis: RRR = relative risk reduction. CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
CAPRIESafety Profile Although the risk of myelotoxicity with clopidogrel appears to be low, this possibility should be considered when a patient receiving clopidogrel has fever or another sign of infection. • Patients with a history of ASA intolerance were excluded from CAPRIE. PLAVIX Prescribing Information. Data on file, Sanofi-Synthelabo Inc.
CAPRIE Tolerability Profile* *ASA-intolerant patients excluded. PLAVIX Prescribing Information. Data on file, Sanofi-Synthelabo Inc.
PAD: When to Refer • Primary care team is not confident making the diagnosis or lacks resources required to make such a diagnosis • Patient has continued symptoms despite a reasonable trial and adherence to best medical therapy • Patient has critical limb ischemia (rest pain, gangrene, or ulceration)
Patient Case Study • 58-year-old Latino male • History of diabetes and hypertension • Treated episodically at local clinic • No current medications • Has taken antihypertensive and oral hypoglycemic agents in the past
Patient Case Study • Physical examination • Height: 5'9″ • Weight: 190 lb • BMI: 28.1 kg/m2 • Waist circumference: 40″ • BP: 168/110 mm Hg • Pulse: 72 bpm BMI = body mass index.
Presenting Symptoms • Presents to the clinic after referral from emergency department where he was evaluated and discharged after an episode of chest pain • Coronary event ruled out by labs and diagnostic studies • Admits that he has never been on medication for more than 3 months at a time • Has no health benefits and works as a construction worker • Does not drink alcohol but smokes 1 pack/day x 30 years • Complains of fatigue and inability to maintain his current productivity at the work site
Laboratory Results • Lipid panel • Total cholesterol: 346 mg/dL • LDL: 170 mg/dL • HDL: 29 mg/dL • Triglyceride: 280 mg/dL • A1C: 9.2% • BUN and creatinine: 19/1.4 mg/dL BUN = blood urea nitrogen; HDL = high-density lipoprotein; LDL = low-density lipoprotein.
Physical Examination • CV: RRR S1 and S2 with no murmurs or gallops • Chest: clear to A/P • Abdomen: rotund, but no pulsatile masses or distention • Vascular: no bruits; upper extremity pulses—normal limits • Lower extremity pulses reveal normal femoral bilaterally • Right popliteal, DP, and PT palpable • Left shows decreased popliteal, DP, and PT • Musculoskeletal: no evidence of foot ulceration or dependent rubor • Neurologic: sensory function intact in upper and lower extremities
? Decision Point What is this patient’s risk category? • High • Moderately high • Moderate • Either moderate or moderately high • Low Use your keypad to vote now!
Therapeutic Considerations • Diagnostic intervention • Evaluate vascular status ABI results • Right = 1.00 • Left = 0.56 • Appropriate management includes: • Control BP • Manage dyslipidemia and diabetes • Initiate antiplatelet therapy • Smoking cessation • Exercise program • Follow-up in 1 month