Download
1 / 19
330 likes | 1.98k Views
Epiglottitis and Croup. By Stacey Singer-Leshinsky R-PAC. Laryngotracheal bronchitis Viral Croup. Known as laryngotracheitis or laryngotracheobronchitis Most common etiology is viral- Parainfluenza virus, adenovirus, RSV . Laryngotracheal bronchitis Viral Croup.

E N D
Epiglottitis and Croup By Stacey Singer-Leshinsky R-PAC
Laryngotracheal bronchitisViral Croup • Known as laryngotracheitis or laryngotracheobronchitis • Most common etiology is viral- Parainfluenza virus, adenovirus, RSV
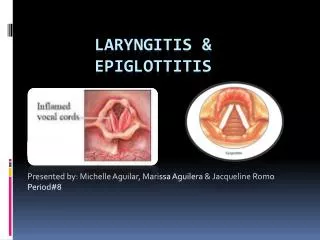
Laryngotracheal bronchitisViral Croup • Leads to infection and inflammation of the larynx and subglottic area • Decreased mobility of the vocal cords • Frequently affects children
Viral Croup Clinical Manifestations • Begins with respiratory symptoms • Within 2 days progresses to: • Hoarseness • Barking seal like cough • Stridor- • Symptoms worse at night • Fever
Viral Croup • Mild disease: occasional barking cough, no stridor at rest, mild to no suprasternal retractions • Moderate: frequent cough, audible stridor at rest, retractions, • Severe: frequent cough, inspiratory/expiratory stridor, retractions, decreased air entry, distress, and agitation.
Laryngotracheal bronchitisCroup-Diagnosis • A/P neck x-ray: subglottic narrowing • CBC might show lymphocytosis-
Croup Differentials • Diphtheria • Epiglottitis • Peritonsillar abscess • Inhalation injuries
Viral Croup-Management • Cool air mist, steam from bathroom, exposure to outdoor cool air • Adequate hydration • Glucocorticoids • Racemic epinephrine • Dexamethasone for severe cases
Viral Croup-Management • Hospitalization indications • Dehydration- • Significant respiratory compromise • Signs of respiratory failure • Complications: • Prognosis:
Spasmodic Croup • No prodrome of upper respiratory syndrome. • Subglottic edema • Affects individual at night. • Affects children between 1-3 years • Managed at home
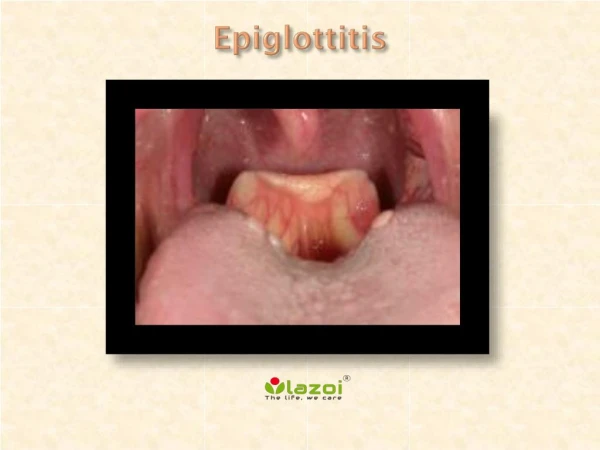
Epiglotittis • The epiglottis is a cartilaginous structure covered with mucous membrane • Epiglottitis is an acute inflammation of the epiglottis and pharyngeal structures • Can be severe life threatening disease
Epiglotittis • Primarily affects children 2-7 years. Presents more acutely in young children • Etiology: H. influenzae type B, also group A S pneumoniae, H parainfluenzae, S aureus, and beta-hemolytic streptococci .
Epiglotittis-Clinical Manifestations • Triad of drooling, dysphagia, and distress. • High fever • Positioning- tripod position • Dyspnea/ Inspiratory stridor/ accessory muscle use / muffled voice • Brassy cough
EpiglottitisDiagnosis • Lateral neck -enlarged edematous epiglottis. • Laryngoscopy: Direct inspection of epiglottis under controlled conditions • Leukocytosis • Blood cultures positive
EpiglotittisDifferentials • Anaphylaxis • Croup • Retropharyngeal Abscess • Foreign body obstruction
EpiglotittisManagement • Secure airway with endotracheal intubation. Might need cricothyroidotomy. • Child should sit upright • Humidified oxygen • Hospitalization • No tongue blades • IV antibiotics:Ceftriaxone (Rocephin) cefotaxime (Ceftin), Ampicillin with chloramphenicol
EpiglotittisManagement • Evaluate for extubation 24-48 hours post intubation. • 24-48 hours post extubation • Rifampin prophylaxis for 4days for household contacts if: children in household have not been vaccinated with the entire series
Review 1 • A 4 year old is brought to the Emergency Room with her mother at 4am. Mother states child is coughing funny. Child has a two day history of an upper respiratory infection. • What is the differential diagnosis? • How would this child be treated? • When would this child be hospitalized? • What findings are expected on neck x-ray?
Review 2 • A 6 year old female is brought to the ED by her father. Father states female is very sick. She is drooling and has a high fever. • What is the differential diagnosis? • What are some other clinical manifestations that might be expected? • How would this child be treated? • Should this child be hospitalized? • What findings are expected on lateral neck x-ray? • What is the etiology of this?