Download
1 / 20
200 likes | 314 Views
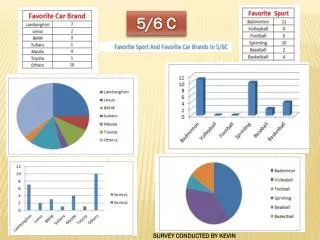
Results of the Jordan medicine price and availability survey conducted in 2004. Presentation Methodology Results Recommendations Activities since 2004. Methodology. Measured medicine prices, availability and affordability using the standardized WHO/HAI methodology Data collected:

E N D
Results of the Jordan medicine price and availability survey conducted in 2004
Presentation • Methodology • Results • Recommendations • Activities since 2004
Methodology Measured medicine prices, availability and affordabilityusing the standardized WHO/HAI methodology Data collected: • Public sector procurement prices • Public sector patient prices & availability • Private sector patient prices & availability Medicine types surveyed: • Originator brand (identified centrally) • Most sold generic equivalent (identified centrally) • Lowest priced generic equivalent (at each outlet) Price components: hypothetical - not measured in the field
Sampling Overall sampling: 18 public sector outlets, 20 private retail pharmacies Public sector procurement datafromMinistry of Health
Medicines surveyed WHO/HAI core list medicines - 23 aciclovir 200mg, amitriptyline 25mg, amoxicillin 250mg beclometasone 0.05mg/dose inhaler, captopril 25mg carbamazepine 200mg, ceftriaxone 1g inj, ciprofloxacin 500mg co-trimoxazole paed susp, diazepam 5mg, diclofenac 25mg fluoxetine 20mg, fluphenazine 25mg/ml inj, glibenclamide 5mg hydrochlorothiazide 25mg, losartan 50mg, metformin 500mg nifedipine retard 20mg, omeprazole 20mg, phenytoin 100mg ranitidine 150mg, salbutamol 0.1mg/dose inhaler Supplementary medicines - 6 diltiazem 60mg, enalapril 20mg, fluconazole 150mg furosemide 40mg, methyldopa 250mg, simvastatin 20mg
Data quality assurance Training workshop for data collectors (pharmacists from Inspection Dept) Data collection forms checked in the field & 10% verified Pre-programmed MS Excel workbook provided with WHO/HAI manual • Data entry checked using 'double entry' function • Workbook’s 'data checker' function used • Automated data analysis Data reviewed by WHO/HAI
Data analysis Affordability Assessed by comparing the cost of medicine treatment, using standard dosing regimens, to the daily wage of the lowest paid unskilled government worker - 3 Jordan Dinar ($ 4.22) / day at time of survey • Acute condition - a week’s course of treatment • Chronic condition - 30 day’s supply Availability Calculated as the percentage (%) of outlets stocking the product on the day of data collection
Prices Calculated as Median Price Ratio (MPR) - local price compared to an international reference price (converted to JD) Management Sciences for Health’s International Drug Price Indicator Guide 2003 used as reference: median prices of high quality generics offered to developing countries in bulk by different suppliers MPR 0.5 means that the local medicine price is half the international reference price MPR 2 means that the local medicine price is twice the international reference price MPR only calculated if medicine found in 4 or more outlets
Examples of medicines with very high prices in private retail pharmaciesoriginator brands and lowest priced generics
Summary of findings Prices • Public procurement prices were acceptable for generics but some higher priced originator brands are being purchased • Public sector patient prices were similar to procurement prices • Private sector patient priceswere extremely high for both originator brands and lowest priced generics Availability very poor in the public sector, much better in the private sector
Summary of findings Affordability • Treatments generally affordable in the public sector but as availability very poor, most people have to purchase medicines from private pharmacies where treatments are less affordable. • Private sector – originator brands not affordable (acute & chronic conditions). Lowest priced generics affordable for some acute conditions but few chronic conditions. Price components cumulative mark-ups thought to be 62-70 import fee charged for most medicines, VAT charged
Recommendations • Review the current pricing policy to ascertain reasons for high medicine prices especially in the private sector but also some high procurement prices • Initiate international tenders and only purchase originator brands where no reasonable alternative or price offered is lowest • Investigate reasons for low availability in the public sector. Supply and demand should be regularly monitored to ensure accurate financing mechanisms to improve funding of essential medicines. • Extend the NHI Scheme to cover the whole population with the aim of lower prices (greater volume; stronger negotiation power for the government) and increased availability
Recommendations • Investigate prescribing and dispensing practices, legalise and encourage generic substitution and educate health professionals and consumers on acceptability of low priced generics • Provide incentives for the dispensing of low priced generics • Abolish taxes on medicines • Regularly monitor prices, availability and affordability & publish results to health professionals and consumers • Conduct a price components field study
Activities since 2004 • New pricing policy developed in January 2004 (prior to survey) and implemented • Some amendments introduced in May 2007