Download
1 / 45
470 likes | 819 Views
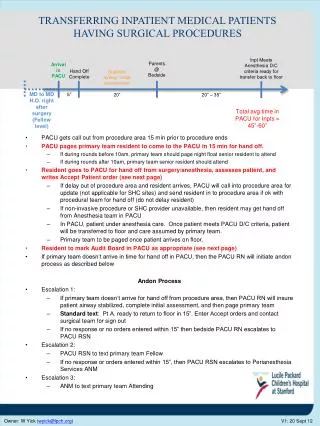
THE ORGANIZATION AND THE ANALYSIS OF THE INPATIENT MEDICAL AID Lecturer: Ph.D., Assosiate Professor Elena A. Abumuslimova. Inpatient medical service history. Inpatient care goes back to 230 BC in India where Ashoka the Great founded 18 hospitals.

E N D
THE ORGANIZATION AND THE ANALYSIS OF THE INPATIENT MEDICAL AIDLecturer: Ph.D., Assosiate Professor Elena A. Abumuslimova
Inpatient medical service history • Inpatient care goes back to 230 BC in India where Ashoka the Great founded 18 hospitals. • The Romans also adopted the concept of inpatient care by building a specialized temple for sick patients in 291 AD on the island of Tiber. From Wikipedia, the free encyclopedia
Inpatient medical service history It is believed the first inpatient care in North America was provided by the Spanish in the Dominican Republic in 1502; the Hospital de Jesús Nazareno in Mexico City was founded in 1524 and is still providing inpatient care. From Wikipedia, the free encyclopedia
Inpatient medical service history Perhaps the most famous provider of inpatient care was Florence Nightingale who was the leading advocate for improving medical care in the mid-19th century. Florence Nightingale 12 May 1820 – 13 August 1910
General characteristic of the inpatient medical aid A hospital is a health care institution providing patient treatment by specialized staff and equipment. There are over 17,000 hospitals in the world.
Levels of the in-patient medical care(1) • Local level – local hospitals, local maternity homes. There is • general type of hospital medical aid in this establishments. • These hospitals serve only local population and carry out • local function. Usually they have branches on therapy, • surgery, obstetric, infectious. • District level – district hospitals, district maternity • home. Here people can receive general and some • kind of specialized type of inpatient medical aid. There are • dermatological, ophthalmologic, otolaryngology, urological • and other branches.
Levels of the in-patient medical care (2) • Regional level – regional hospitals. There are • general, specialized and highly tailored type of inpatient • medical aid in this establishments. These hospitals carry out • local, intermediate and regional functions, cover the big • territory with wide spectrum of the specialized help • (modern cancer therapy, chest surgery, cardiology, etc.). • Federal level – medical establishments caring out only some • kind of highly tailored and unique type of inpatient medical • aid. Its may be scientific-research establishments, medical • centers.
Levels of the in-patient medical care (3) • Rural hospitals form the separate group. They play a role of the elementary medical and hospital centre in the remote villages.
Types of the inpatient medical care: • Primary (general) • Secondary (specialized) • Tertiary ( highly tailored)
General characteristic of the inpatient medical aid (1) • Organizational forms of rendering of the in-patient services to the population, structure of hospital establishments and their accommodation depend on: • morbidity level among population on the territory; • disease structure of the population; • age-sexual structure of the population; • features of residence.
General characteristic of the inpatient medical aid(2) The hospital medical aid is carried out at the heaviest diseases demanding application of complex methods of diagnostics, therapeutic treatment, operative intervention, constant medical supervision and qualified care. This is the most expensive type of medical aid but the most effectiveness from the medical and social point of view.
Reasons for hospitalisation: • the case of diseases requiring a comprehensive approach to diagnosis and treatment; • the use of complex methods for examination • treatment with the using of modern high-tech medical equipment; • surgery; • continuous round-the-clock medical supervision and intensive care.
Negative reasons for inefficient using of hospital in Russia • inadequate extension hospital beds; • high rates of inappropriate and non-core hospitalization; • inadequate increase of terms of stay of the patient in the hospital; • hospitalization of patients in unprepared to provide a profile of medical aid medical institutions; • high frequency of transfers of patients from one medical facility (the unprepared or non-core) to another.
Optimisation hospital services in Russia(1) • Implementation stages of medical care on the basis of rational distribution of functional duties hospitals: • - municipal (city and district) – to provide primary care in emergency cases;- inter-district - for specialized assistance, including emergency cases and conditions requiring treatment and rehabilitation;- federal - to provide specialized including high-tech service
Optimisation hospital services in Russia (2) • 2. Introduction to the clinical departments of hospitals: • disease management protocols and standards of care; • registers for hospital patients; • health care quality management system.3. Installation and stuffing of hospitals with qualified personnel according to approved standards.
Optimisation hospital services in Russia (3) 4. Expansion of volumes and the introduction of new types of high-tech medical assistance.5. Round-the-clock telemedicine links between municipal and regional level hospitals. 6. To intensify the work of hospital beds through the introduction of hospital-replacing diagnostic technologies at the outpatient level and organization of gradual rehabilitation (medical attendance service, the system aftercare and rehabilitation).
Optimisation hospital services in Russia (4) 7. Improvement of the tariff policy, based on the consideration not only of the type and amount of medical assistance, but also on its quality;8. Improvement aims of the hospital work reflecting the quality of medical aid (lethality rate, the degree of restoration of the disturbed functions).
Classification of in-patient establishments (1) Depending on a bed capacities hospital are divided into categories. Very large and very small hospitals are considered to be not included into any category. (Lisitcyn J.P., Kopit N.J., 1984 classification)
Classification of the in-patient establishments (2) • Depending on a kind there are: • multifield hospitals • specialized hospitals • dispensaries
Classification of the in-patient establishments (3) • Due to the regulations of hospitalization there are: • first aid hospitals • hospital for list hospitalization • hospital for the general (mixed) hospitalization.
Classification of the in-patient establishments (4) • According to the system of their organization there are: • united with polyclinic hospitals • non-united with polyclinic hospitals. • For the district, regional and federal hospitals presence of polyclinic as a structural part is always obligatory.
Functions of the in-patient establishments by WHO • Function of hospital establishments are dynamic concepts and depend on the tasks set at the given stage of development of public health services. • The WHO suggested to systematize functions of modern hospital in four groups: • rehabilitation & treatment (diagnostics and treatment of diseases, rehabilitation and urgent medical aid); • preventive, especially for hospitals united with a polyclinic (medical-improving activity, prevention of infectious and chronic diseases, disablement); • education (training of medical personnel and its post-diploma specialization); • research.
Hospital structure • Management department: the head-physician, his deputies (for medical department, polyclinic, medical working capacity examination), medical statistics department, medical archive, accounts department, library, etc. • reception department • medical (curative) department (surgical, therapeutic, • neurological, urological, etc.) • the specialized medical departments (physiotherapeutic, • exercise therapy, massage, etc.), • separate diagnostic services (it includes different laboratories, • rooms – electrocardiographic, x-ray, etc.) • drugstore, • department of morbid anatomy, • maintenance department (nutrition unit, storehouses, laundry, • technical department, transport, etc.)
Organization principles of work of the hospitals :medical care of the in-patient establishments • Direct treatment of patients is executed by doctors - interns, which basic elements of work are carrying out the inpatient case record, diagnostics and treatment, examination of work capacity, rehabilitation and regenerative treatment, consultations. • Load of hospital doctor is about 20-25 patients.
The basic registration documents • a medical card of the inpatient (case history; registration form № 003/y) • a discharge card (form № 055/y) • a register of operations (form № 008/y) • a register of reception of patients and refusals from hospitalization (form № 001/y) • form for the daily account of patients and beds fund (form № 007/y) • a register of medical autopsy (form № 012/y)
The basic accounting documents • Data on treatment-and-prophylactic establishment (the annual report, form № 30) • Data on the medical and pharmaceutical staff (form № 17) • Data on activity of a hospital (form № 14) • Data on activity of the treatment-and-prophylactic establishments working in a system of OMI for certain year (form № 52) • Data about bed fund and its use for 12 month period
An analysis of activity of inpatient medical service • More than 100 different parameters of inpatient medical aid are widely used. All parameters can be grouped, since they reflect certain directions of functioning of hospital: • supply of the population with inpatient aid; • load of the medical staff; • material and medical equipment; • use of bed fund; • completeness of medical staff; • quality of the inpatient medical aid and its efficiency
The main quantitative indicators of hospital activity Provision of the population with the hospital medical help Load of medical personnel Material-technical medical equipment Indicators use bed facility Indicators of staffing
The main qualitative indicators of hospital activity • Hospital lethality • The proportion of patients fully or partially regained the functional independence and ability to work among all treated patients. • Level of postoperative complications. • The structure of outcomes of hospitalisation, etc.
An analysis of quality of treatment in a hospital^parameters of bed fund use • mean annual occupation of bed (average occupation of a bed for municipal hospital is 330-340 days, for rural hospitals – 300-310 days; for municipal maternity homes – 300-310 days, for rural maternity home – 280-290 days); • mean duration of patient’s stay in a hospital – from 17 to 19 days (causes of long-lasting treatment in a hospital: severity of disease, late diagnostics of diseases, cases when patients aren’t prepared for hospitalization – not examined, etc.); • bed turnover is one of the major parameter of efficiency of bed fund use (mean number of patient is 17-20 and more patients) • a mean idle time of a bed; • dynamics of bed fund
Planning for inpatient care Health planning is a well-grounded calculation of the network of health care establishments, their staffs, medical network, indicators of use of the bed facility, financial and material support.
The required basic data for planning 1. Data about the level of public health;2. Information about existing network of medical institutions, staffs and public health establishments;3. Information about economic situation of the district, future prospects of its development;4. Assessment of sanitary-epidemiological conditions in the region;
General characteristic of the inpatient medical aid Approximate standard for the inpatient medical aid to the population (per 1000 people)
The density of hospital beds The density of hospital beds in the adult population in Russia is on average of 13.2 beds per 1000 inhabitants, child (up to 18 years) - 9 beds per 1000 children.
Medical care for rural population
The organization of medical aid to rural population • The factors that determined organizational forms and methods of work of rural medical institutions: • character of spreading of the population, • area of coverage, • seasonal prevalence of works, • influence of weather conditions at the field works, • specific conditions of labor process, • disorder of economic - household activity and conditions of life, • regional and national features and customs, • educational and cultural level, etc.
Factors affecting the organisation of medical care for rural people • the distance of medical institutions from the residence of patients, • enough qualified personnel and the equipment, • opportunities to receive specialized medical aid, • opportunity for realisation of specifications of medico-social security.
Three stages of medical care to rural population Rural medical outpost or territorial medical associations (local hospital, paramedical and obstetrical outposts, health centers, maternity hospitals, a day nursery - kinder gardens, etc.). At this stage rural population receive the qualified medical aid; District level, where the main establishment is the central district hospital. Rural population receives the qualified specialized medical aid of basic kinds. Regional hospital, clinics, dentist polyclinic, regional territorial sanitary-epidemic management establishment, etc. At this stage is implemented a highly skilled medical aid on all specialities.
Structure of a primary link of medical aid to rural population The rural paramedical-obstetric outpost is a link of first patients contact in system of health services. Its primary goals are rendering the pre-medical help and carrying out sanitary-antiepidemic actions directed on prophylaxis of diseases, decrease in morbidity and traumas, increase of sanitary and hygienic culture of the population. Paramedical staff renders the first medical aid at acute conditions and traumas, carry out vaccination, physiotherapeutic actions, etc. Paramedical and obstetrical outposts are organized in settlements where number of inhabitants varies from 700 up to 1000
Structure of a primary link of medical aid to rural population The basic medical institution on a rural medical outpost is the local hospital or polyclinic. Character and volume of medical aid in local hospital basically are determined by its capacity, equipment and presence of doctor-experts. The number of staff of rural hospital is depending on its capacity, population and distances up to central regional hospital, there have to be doctors of the basic specialities (therapy, pediatric, stomatology, obstetrics, gynecology and surgery).
Duties of local hospital doctor • Treatment of therapeutic and infectious patients • Deliveries medical aid • Treatment-and-prophylactic help to children • Urgent surgical and traumatological help
Structure of secondary link of medical aid to rural population The main link in public health service of rural area is central regional hospital (CRH), which carries out the specialized medical aid by its basic kinds and an organizational - methodical management of all medical institutions of area. In its structure CRH has the following divisions: hospital with the basic specialized branches, polyclinic with advisory receptions of doctors - experts, medical - diagnostic branches, organizational -methodical cabinet and other structural divisions (mortuary, mess, pharmacy, etc.).
Thank you for your attention!