Download
1 / 52
560 likes | 1.01k Views
Exercise Treadmill Testing. Prognostication in Coronary Artery Disease Dr. Peter Krampl 11 October 2001. Introduction. 300,000 ER visits per year acute non traumatic chest pain Only apx. 25% have clear positive, Unstable coronary disease Angiography Image studies

E N D
Exercise Treadmill Testing Prognostication in Coronary Artery Disease Dr. Peter Krampl 11 October 2001
Introduction • 300,000 ER visits per year acute non traumatic chest pain • Only apx. 25% have clear positive, • Unstable coronary disease • Angiography • Image studies • Acute myocardial infarction • or negative diagnosis of coronary syndromes
Introduction • Current ED Modalities • Reviewed in EM Clinics February 2001 • History / Physical • Mair. Chest. 1995. • 110 patients; non traumatic chest pain • Using NPV as most used indicator for admission • PPV 53% NPV 75% for acute cardiac ischemia
Introduction • Current ED Modalities • ECG • Rovan, American Journal Cardiology. 1989. • Multicentre Chest Pain Trial • Sensitivity 61% Specificity 90% for ischemia • Current ST, Q, LBBB criteria • Variable Specific • Addition of T wave abnormality • Sensitivity increases to 95% • Specificity may decreases to 23% • Current computer algorithms tend to higher sensitivity
Introduction • Current ED Modalities • Cardiac Markers • Hedges et al. Acad EM. (CK-MB) • 1042 patients; CK-MB at presentation and serial investigated • Sensitivity 19-31% Specificity 95-96% • Hamm et al. NEJM. 1997 (TnT) • 776 patients • Prospective study looking at prognosis of TnT and TnI and 30 day cardiac event rate • Negative values of T and I gave annual event rates of 1.1 and 0.3% respectively • Sensitivity 31% Specificity 98%
Introduction • Are We Satisfied With Those Numbers? • How Do We Further Risk Stratify Coronary Patients? • Treadmill Testing • Observation Units / Time • Radionuclear Imaging +/- Exercise • Echocardiography +/- Exercise • Angiography
Introduction • In ED, old chart or patient notes: • I was on treadmill for 8 minutes. • A negative treadmill. • I did not have pain on the treadmill. • What do those mean? • Can we use those simple guides to further stratify these patients?
Outline • Introduction • Treadmill Testing • Review of Current Literature • Introduction • Indications • Procedures • Results • Notable Studies • Exercise Modalities • Conclusions • Questions
Treadmill Testing: Introduction • Froelicher. Hdbk of Exercise Testing. 1996 • Goals • Diagnosis CAD • Prognosis CAD • Evaluation of Medical Therapy • Evaluation of Exercise Capacity
Treadmill Testing: Indications • When to use…. • AHA / CPSA guidelines advise to use only up to intermediate pre test probability cases • Kuntz et al. Ann Int Med. 1999. • Exercise stress test or rest echo most cost effective (mild-mod) • Life expectancy • Cost • Incremental Cost Effectiveness over other modalities • For high risk, immediate coronary angio most cost beneficial. • Other stress modalities supplement to Exercise Treadmill
Treadmill Testing: Indications • Braunwald et al. High / Intermediate / Low Risk / Pretest Probability Guidelines published by AHA 1995. Reviewed by Primary Care Clinics. 2001 • Example: Low Risk • Chest pain by history classified as “probable not or definitely not angina • normal ECG • New onset angina 2 months • No change in previous 2 months • T wave flattening or inversion <1 mm in leads with dominant R waves • One risk factor other than diabetes
Treadmill Testing: Indications • Majority of tests done on referral basis • Advent of chest pain units in United States… • Studies by • Zalenski. Ann EM. 1997. Low and Intermediate Risk. • Safety at 4-12 hours • Mikhail. Ann EM. 1997. Intermediate risk. • Safety at 12 to 24 hours • Lewis. Am J Card. 1994. Low risk. • Safety at 1-2 hours • Kirk. Ann EM. 1998. Low risk. • Safety at 1-2 hours • CP Observation Units have adopted 6 hours as Industry standard for exercise port work up and stabilization
Treadmill Testing: Indications • Indications • Froelicher / Annals of EM • Clear (Class 1) • Evaluation of male patients with atypical symptoms • Functional capacity testing • Evaluation of exercise related dizziness, syncope, palpitations • Evaluation of Recurrent exercise induced Arrhythmias
Treadmill Testing: Indications • Indications • Probable Benefit (Class 2) • Evaluation of Women with atypical symptoms • Evaluation of Variant Angina • All those in Class one with baseline ECG changes other than LBBB • Evaluation of patients on digitalis or RBBB
Treadmill Testing: Indications • Indications • Not Indicated (Class 3) • Assymptomatic young men / women with no risk factors and high suspicion non cardiac chest discomfort • Evaluation of patients with LBBB • Evaluation of Patients with Pre-excitation Syndromes
Treadmill Testing: Indications • Contraindications • AHA Guidelines • Absolute • AMI within 3-5 days • Unstable angina not stabilized by medical therapy • Aortic dissection • Endo, Myo, or pericarditis • PE • Lower Extremity Thrombosis • Uncontrolled symptomatic cardiac arrhythmias • Severe aortic stenosis • Symptomatic severe and terminal heart failure
Treadmill Testing: Indications • Contraindications • Relative • High degree AV block • Moderate stenotic valvular disease • DBP >200 or DBP > 110 • Bradyarrythmias • Known left main coronary stenosis • Mental / physical incapacity
Treadmill Testing: Indications • Complications • Brady / Tachyarrythmias • AMI / Sudden Death • CHF / Shock • MSK Trauma / Fatigue / Malaise
Treadmill Testing: Procedures • Important Concepts • VO2 max : maximum oxygen uptake • Amt of O2 transported for cellular metabolism • Useful to express in multiples of METS • CO X (arteriovenous oxygen difference) • METS used to standardize protocols • MO2 : myocardial O2 uptake • wall tension, thickness, contractility and HR • Estimated by double product (HR X BP) • Angina usually occurs at the same double product
Treadmill Testing: Procedures • Physiology • Exercise creates increase CO • Four to six fold increase from rest at peak • CO increase by increase HR and PB and decreased vagal tone • HR affected by • Age, sex, motivation, habitus, blood volume, health • SBP increases with exercise • DBP stays same or slightly decreases • Hypotension ominous sign • Outflow obstruction, ventricular dysfunction or ischemia
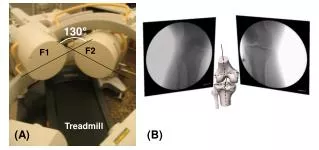
Treadmill Testing: Procedures • Equipment • Treadmill or cycle ergometer • Cycle has major pitfall of rapid fatigue of quadriceps in older patients • Most studies use treadmill • Handrails, Rest Area • Assistant, Supervisor • Resuscitation Equipment
Treadmill Testing: Procedures • Preparation • Fast 3 hours prior / dress appropriately… footwear • Medications reviewed by physician prior • History and physical prior regarding change in disease • CHF; valvular disease; onset of unstable angina; bronchospasm • Consent • Baseline supine and upright ECG
Treadmill Testing: Procedures • Protocols • Most diagnostic and prognostic studies based on Bruce protocol • Seven phases • Change in grade and speed every 3 minutes • Correlation with METS • Large incremental stages • Not correlated for height / weight / stride • Ideal protocol lasts 6-12 minutes and adjusts for patients ability • Others include Naughton, McHenry, USAF, Blake
Treadmill Testing:Procedures • Borg Scale • Borg. Sports and Exercise. 1982. • Correlation of scale to actual fatigue • 6-20 grade scale for exertion • 10 grade scale for exertion now adopted • 0 – nothing • 9 – very strong • 10 – very, very strong • Continues to be a clinical assessment of fatigue by technician (skilled) and supervisor • Mainly used as repetitive assessment tool in rehab
Treadmill Testing: Procedures • Measurements • ST depression / elevation (60-80 ms; J point changes) • ST slope (downsloping worse than horizontal) • Duration of changes into recovery • Exercise induced arrhythmias • Peak HR / BP • Total Duration • Exertional hypotension • Angina • Other exercise induced symptoms
Treadmill Testing: Procedures • Termination • Absolute • Drop of SPB > 10 • Anginal Pain (other than non-limiting / known pain) • CNS symptoms • Signs of poor perfusion • Serious Arrhythmias (runs of VT > 3; multiform) • Technical Difficulties in monitoring • Subject Request
Treadmill Testing: Procedures • Termination • Relative • Maintenance of SBP well into protocol • Excessive ST / QRS changes • Fatigue, SOB, Wheeze, Cramps, Claudication • SVT • Development of BBB • Observation Important !! • Case 77 y.o. male; level one indications; no contraindications; stable angina • Maintenance of SBP into Phase 2
Treadmill Testing: Results • Diagnostic • Exercise Treadmill (ST response only) Sens 66% Spec 84% Froelicher et al. Exercise. 1993. Sens 70% Spec 75% Gianrossi. Meta-analysis. Circulation. 1989. Using Bayes rules of pretest probability, these numbers may only be applied to intermediate cases at best. • Original Duke University Investigators showed repeated studies of poor specificity and positive predictive value
Treadmill Testing: Results • Diagnostic • Lehmann and Froelicher. Veteran’s Study Group. QUEXTA. Ann Int Med. 1998. • 814 patients • 400 selected for decreased work-up bias • Only 40% Stress test ‘positive’ ST changes correlated to > minimal luminal CAD • Overall sensitivity 45% specificity 85%
Treadmill Testing: Results • Prognostic • Giagnoni. NEJM. 1983 • Prospective following of 135 men with ST changes vs. 379 controls • Angina, MI, sudden death endpoints • 5.55 percent risk increase • Suggested that ECG positive ST changes should be independent coronary risk factor
Treadmill Testing: Results • Prognostic • Mark et al. Duke University. Ann Int Med 1987; • Validation Mark et al. NEJM. 1991. • Developed score based on 613 patients (1983-85) • Validated on further 1420 patients • Simple score to prognosticate patients • Associated score > 5 with annual mortality of • 0.25 % outpatients • 0.6 % inpatients
Treadmill Testing: Results • Prognostic • Duke Score • Time in minutes • ST depression in mm • Type of pain 0 - none 1 – typical anginal pain limited by time / fatigue / other 2 – limiting anginal pain
Treadmill Testing: Results Duke Score = Time(m) – 4X Angina – 5X depression(mm) Score: 5 & above low risk 4 to –9 intermediate risk -10 & below high risk
Treadmill Testing: Results • Kowk et al. JAMA. 1999. • Revisited Duke Score • 2405 patients • 939 had ST segment changes on stress test • Found 97 % seven year survival based on score Duke > 5 • These studies have solidified the prognostic benefits of the treadmill test
Treadmill Testing: Results • Duke score • Low Risk • Less than 1% per year acute coronary syndrome • Optimize Medical Rx; reassess in one year • Intermediate Risk • 1 to 5 % per year • Optimize Medical Rx; nuclear studies non-urgent • High Risk • Greater than 5 % per year • Urgent referral for further risk stratification
Treadmill Testing: Results • Other prognostic indices: • Morrow & Froelicher. Ann IM. 1993. • Veteran’s Score • Exercise duration • ST depression • Rate of change of systolic BP during exercise • History of CHF, digoxin use • Low risk groups stratified with 2% annual mortality
Treadmill Testing: Results • Exercise Capacity • AHA Guidelines • Carliner et al. Am J Card. 1985 • Reasonable to Use exercise testing for • Surgical patients recovering from • Congenital repair • Valvular replacement • Cardiac transplant • CHF • DM • CRF • Chronic Lung Disease • No exercise induced symptoms
Treadmill Testing: Results • Exercise Capacity and Prognostication • Lauer and Fletcher. Circulation. 1996. • 1575 men; mean age 43 • Failure to achieve 85 % of age predicted maximum heart rate • associated with increase in death of 1.84 • Extrapolation techniques used
Treadmill Testing: Results • AHA Guidelines • Evaluation of Medical Therapy • Look for improvement of exercise capacity to previous before angina or ST depression • Evaluation of Valvular Disease • Strict guideline for evaluation of AS • Evaluation of Dysrrythmias • PVC, Sick sinus Syndrome • Pre-operative • Anesthetists 2nd largest user of stress test for evaluation of patient for non cardiac surgery
Notable Studies • Exercise Hypotension • Dubach et al. Circulation. 1989 • Looking at SBP drop with exercise • Looked at 0, 10, 20 drop of SBP • Drop of 20 associated with increased PPV of at least 50% Left Main or Triple Vessel Disease
Notable Studies • Variables • Prakash et al. Am Heart J. 2001 • 3974 men • Kaplan-Meier regression • Four variables predict mortality within 5 year • Rate of change of rate-pressure product • Age > 65 • Maximum MET <5 • LVH on ECG
Notable Studies • METS • Ramamurthy et al. Chest. 1999. • Found that sensitivity increases if MET >7 • Also found that METS achieved may be a stronger variable than rate-pressure product • High heart rate at low MET (<5) level carries adverse prognosis
Notable Studies • Risk Factors • Am J Cardiol. MRFIT. 1985. • Multiple Risk Factor Intervention Trial • 12,866 participants • Those with ST changes on Stress Treadmill benefit to greater degree with risk factor modification than controls.
Notable Studies • Women • Large number of false positives • Mitral valve prolapse; • Higher incidence atypical chest pain • Hormonal, esp. estrogen mimickery of digoxin • Ventilation Responses and Metabolic Alkalosis • Curzen. Heart. 1998. • 205 women • Compared with coronary angiography • 42 false positives & 31 false negatives (36 % of total) • Increase false positives correlated with • Increasing age to 52 • Increasing coronary risks to 3
Notable Studies • Early Stress Testing • Polanczyk. Am J Card. 1998. • 276 low risk patients • Stress test within 48 hours • Similar prognostication numbers • 0.5 % event rate • Additional variables over 6 months • 15% less ED visits • 30% fewer admission
Exercise Modalities • Stress Echocardiography • Evaluate rest / stress changes in wall motion. • Dobutamine given to stimulate beta-1 • Advantages: Readily available; little equipment; transportable • Disadvantages: poor images in up to 10%; user dependant; hard in presence of previous abnormalities
Exercise Modalities • Thallium 201 • Older agent; Replaces potassium in cells • Advantages • Able to calculate lung heart ratios • Disadvantages • Immediate imaging • Poor in obese patients and large breasted women • Maddahi. Am J Coll Card. 1989 • Increases sensitivity from 60-70% of treadmill test to 90% overall with addition of perfusion studies but 70% with single vessel disease
Exercise Modalities • Technetium-99m sestamibi • Deposited into mitochondria • Advantages • Longer half life • Better images • Improved estimates of ejection fraction • Disadvantage • Poor extraction from blood at high blood flow • Hachamovitch et al. Circulation. 1996. • 834 patients; treadmill, Tc-99m and catheterization • 78% of the listed 0.6% mortality from Duke Low Treadmill prognostication caught as severe perfusion scans.
Exercise Modalities • Two schools of thought: • EM Clinics Feb 2001 • “as useful as exercise testing is, it has the limitations of suboptimal sensitivity and specificity…. Imaging is a necessity, not an optional component of stress testing” vs. “exercise testing alone is a useful first step.” • Froelicher. Primary Care. 2001. • Quotes George Bernard Shaw “the doctor does the test he is paid the most for” to stress our need for continued evaluation of present modalities