Download
1 / 1
10 likes | 144 Views
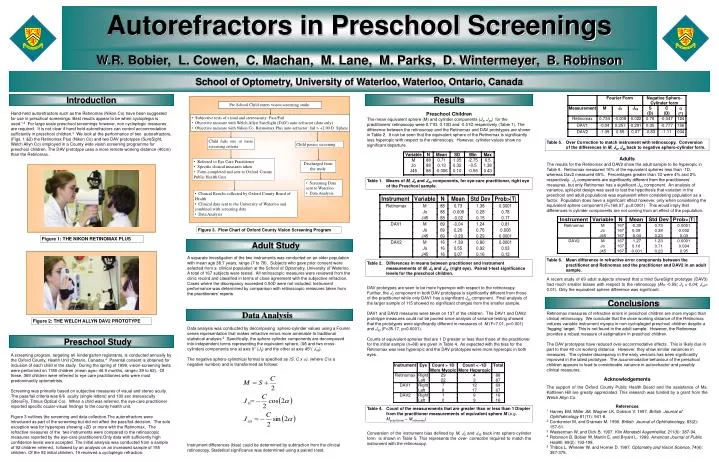
Autorefractors in Preschool Screenings. W.R. Bobier, L. Cowen, C. Machan, M. Lane, M. Parks, D. Wintermeyer, B. Robinson. School of Optometry, University of Waterloo, Waterloo, Ontario, Canada. Introduction. Results. Pre School Child enters vision screening study:.

E N D
Autorefractors in Preschool Screenings W.R. Bobier, L. Cowen, C. Machan, M. Lane, M. Parks, D. Wintermeyer, B. Robinson School of Optometry, University of Waterloo, Waterloo, Ontario, Canada Introduction Results Pre School Child enters vision screening study: Hand-held autorefractors such as the Retinomax (Nikon Co) have been suggested for use in preschool screenings. Best results appear to be when cycloplegia is used.1,2 For large scale preschool screenings however, non cycloplegic measures are required. It is not clear if hand held autorefractors can control accommodation sufficiently in preschool children.3We look at the performance of two autorefractors, (Figs. 1 &2) the Retinomax Plus (Nikon Co) and two DAV prototypes (SureSight, Welch Allyn Co) employed in a County wide vision screening programme for preschool children. The DAV prototype uses a more remote working distance (40cm) than the Retinomax. Preschool Children The mean equivalent sphere (M) and cylinder components (J0, J45) for the practitioners’ retinoscopy were 0.71D, 0.13D and -0.01D respectively (Table 1). The difference between the retinoscopy and the Retinomax and DAV prototypes are shown in Table 2. It can be seen that the equivalent sphere of the Retinomax is significantly less hyperopic with respect to the retinoscopy. However, cylinder values show no significant departure. • Subjective tests of visual and stereoacuity: Pass/Fail • Objective measure with Welch Allyn SureSight (DAV) auto-refractor (data only) • Objective measure with Nikon Co. Retinomax Plus auto-refractor: fail > +2.00 D Sphere Child fails one or more screening criteria Table 5. Over Correction to match instrument with retinoscopy. Conversion of the differences in M, J0, J45 back to negative sphero-cylinder form. Child passes screening Adults The results for the Retinomax and DAV2 show the adult sample to be hyperopic in Table 6. Retinomax measured 16% of the equivalent spheres less than -1D, whereas Dav2 measured 65%. Percentages greater than 1D were 4% and 2% respectively. J0 components are significantly different from the practitioners’ measures, but only Retinomax has a significant J45 component. An analysis of variance, split-plot design was used to test the hypothesis that variation in the preschool and adult populations was equivalent when considering population as a factor. Population does have a significant effect however, only when considering the equivalent sphere component (F=168.07, p=0.0001). This would imply that differences in cylinder components are not coming from an effect of the population. • Referred to Eye Care Practitioner • Specific clinical measures taken • Form completed and sent to Oxford County Public Health Unit Discharged from the study Table 1. Means of M, J0 and J45 components, for eye-care practitioner, right eye of the Preschool sample. • Screening Data sent to Waterloo • Data Analysis • Clinical Results collected by Oxford County Board of Health • Clinical data sent to the University of Waterloo and combined with screening data • Data Analysis Figure 3. Flow Chart of Oxford County Vision Screening Program Figure 1: THE NIKON RETINOMAX PLUS Adult Study A separate investigation of the two instruments was conducted on an older population with mean age 38.7 years, range (7 to 78). Subjects who gave prior consent were selected from a clinical population at the School of Optometry, University of Waterloo. A total of 167 subjects were tested. All retinoscopic measures were reviewed from the clinic record and classified in terms of close agreement with the subjective refraction. Cases where the discrepancy exceeded 0.50D were not included. Instrument performance was determined by comparison with retinoscopic measures taken from the practitioners’ reports. Table 6. Mean difference in refractive error components between the practitioner and Retinomax and the practitioner and DAV2 in an adult sample. Table 2. Differences in means between practitioner and instrument measurements of M, J0 and J45 (right eye). Paired t-test significance levels for the preschool children. A recent study of 69 adult subjects showed that a third SureSight prototype (DAV3) had much smaller biases with respect to the retinoscopy (M= -0.58; J0 = 0.04; J45= 0.01). Only the equivalent sphere difference was significant. DAV prototypes are seen to be more hyperopic with respect to the retinoscopy. Further, the J0 component in both DAV prototypes is significantly different from those of the practitioner while only DAV1 has a significant J45 component. Final analysis of the larger sample of 115 showed no significant changes from the smaller sample. DAV1 and DAV2 measures were taken on 137 of the children. The DAV1 and DAV2 prototype measures could not be pooled since analysis of variance testing showed that the prototypes were significantly different in measures of M (F=7.01, p=0.001) and J45 (F=35.17, p=0.0001). Counts of equivalent spheres that are 1 D greater or less than those of the practitioner for the initial sample (n=88) are given in Table 4. As expected with the bias for the Retinomax was less hyperopic and the DAV prototypes were more hyperopic in both eyes. Conclusions Data Analysis Retinomax measures of refractive errors in preschool children are more myopic than clinical retinoscopy. We conclude that the close working distance of the Retinomax induces variable instrument myopia in non-cyclopleged preschool children despite a ‘fogging’ target. This is not found in the adult sample. However, the Retinomax provides a robust measure of astigmatism in preschool children. The DAV prototypes have reduced over-accommodative effects. This is likely due in part to their 40 cm working distance. However, they show similar variances in measures. The cylinder discrepancy in the early versions has been significantly improved in the latest prototype. The accommodative behaviour of the preschool children appears to lead to considerable variance in autorefractor and possibly clinical measures. Figure 2: THE WELCH ALLYN DAV2 PROTOTYPE Data analysis was conducted by decomposing sphero-cylinder values using a Fourier series representation that makes refractive errors more amenable to traditional statistical analysis.5 Specifically, the sphero-cylinder components are decomposed into independent terms representing the equivalent sphere, (M) and two cross-cylinders components one at axis 0 (J0) and the other at axis 45(J45). The negative sphero-cylindrical format is specified as (S, C x ), (where C is a negative number) and is transformed as follows: Preschool Study A screening program, targeting all kindergarten registrants, is conducted annually by the Oxford County, Health Unit (Ontario, Canada).4 Parental consent is obtained for inclusion of each child in the study. During the spring of 1999, vision-screening tests were performed on 1180 children (mean age= 46.9 months, range= 39 to 62). Of these, 369 children were referred to eye care practitioners who were most predominantly optometrists. Screening was primarily based on subjective measures of visual and stereo acuity. The pass/fail criteria was 6/6 acuity (single letters) and 100 sec stereoacuity (SteroFly, Titmus Optical Co). When a child was referred, the eye-care practitioner reported specific ocular-visual findings to the county health unit. Figure 3 outlines the screening and data collection.The autorefractors were introduced as part of the screening but did not affect the pass/fail decision. The sole exception was for hyperopes showing +2D or more with the Retinomax. The refractive measures of the two instruments were compared to the retinoscopic measures reported by the eye-care practitioners.Only data with sufficiently high confidence levels were accepted. The initial analysis was conducted from a sample of 92 children referred, followed by an analysis on an increased sample of 155 children. Of the 92 initial children, 19 received a cycloplegic refraction. Acknowledgements The support of the Oxford County Public Health Board and the assistance of Ms. Kathleen Hill are greatly appreciated. This research was funded by a grant from the Welch Allyn Co. References 1 Harvey EM, Miller JM, Wagner LK, Dobson V. 1997. British Journal of Ophthalmology 81(11): 941-8. 2 Cordonnier M, and Dramaix M. 1998. British Journal of Ophthalmology, 83(2): 157-61. 3 Wasserman W, and Dick B. 1997. Klin Monatsbl Augenheilkd, 211(6): 387-94. 4 Robinson B, Bobier W, Martin E, and Bryant L. 1999. American Journal of Public Health, 89(2): 193-198. 5 Thibos L, Wheeler W, and Horner D. 1997. Optometry and Vision Science, 74(6): 367-375. Table 4. Count of the measurements that are greater than or less than 1 Diopter from the practitioner measurements of equivalent sphere M (e.g. Mpractitioner – Mretinomax) Conversion of the instrument bias defined by M, J0 and J45 back into sphero-cylinder form is shown in Table 5. This represents the over- correction required to match the instrument with the retinoscopy. Instrument differences (bias) could be determined by subtraction from the clinical retinoscopy. Statistical significance was determined using a paired t-test.