Download
1 / 1
10 likes | 166 Views
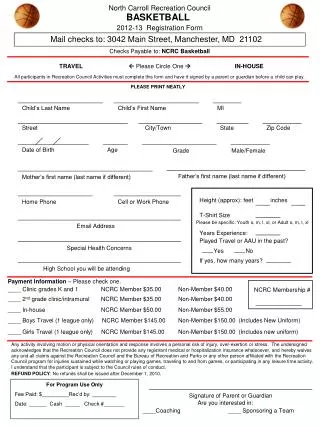
North Carroll Recreation Council. BASKETBALL. 2009 Registration Form. Mail to: NCRC Basketball, 3020 Crown Circle; Manchester, MD 21102. Checks Payable to: NCRC Basketball. TRAVEL Please Circle One INTRAMURAL.

E N D
North Carroll Recreation Council BASKETBALL 2009 Registration Form Mail to: NCRC Basketball, 3020 Crown Circle; Manchester, MD 21102 Checks Payable to: NCRC Basketball TRAVEL Please Circle One INTRAMURAL All participants in Recreation Council Activities must complete this form and have it signed by a parent or guardian before a child can play. PLEASE PRINT NEATLY Child’s Last Name Child’s First Name MI Street City/Town State Zip Code Date of Birth Age Grade (2009-2010) Male/Female Father’s first name (last name if different) Mother’s first name (last name if different) Height (approx): feet inches Home Phone Cell or Work Phone T-Shirt Size Please be specific: Youth s, m, l, xl, or Adult s, m, l, xl Email Address Years Experience: Played Travel or AAU in the past? Special Health Concerns Yes No Please circle any days you are unableto practice. We will do our best to help, but sometimes we cannot accommodate. If yes, how many years? Mon Tue Wed Thu Fri Payment Information – Please check one. ____ Clinic grades K and 1 NCRC Member $30.00 Non-Member $35.00 NCRC Membership # ____ 2nd grade clinic/intramural NCRC Member $45.00 Non-Member $50.00 ____ Intramural NCRC Member $45.00 Non-Member $50.00 ____ Boys Travel NCRC Member $180.00 Non-Member $185.00 (submit Intramural Fees only) ____ Girls Travel NCRC Member $150.00 Non-Member $155.00 (submit Intramural Fees only) Any activity involving motion or physical orientation and response involves a personal risk of injury, over-exertion or stress. The undersigned acknowledges that the Recreation Council does not provide any registrant medical or hospitalization insurance whatsoever, and hereby waives any and all claims against the Recreation Council and the Bureau of Recreation and Parks or any other person affiliated with the Recreation Council program for injuries sustained while watching or playing games, traveling to and from games, or participating in any leisure time activity. I understand that the participant is subject to the Council rules of conduct. REFUND POLICY: No refunds shall be issued after December 1, 2008. For Program Use Only Fee Paid: $_________Rec’d by: ________ Date: ______ Cash _____ Check #_______ Evaluation (circle): YES NO Signature of Parent or Guardian Are you interested in: ____Coaching ____Team Mom/Dad ____ Sponsoring a Team