Download
1 / 20
210 likes | 444 Views
ROCKET- AFology The Pharmacist look-alike Jeopardy G ame Based on the ROCKET-AF TRIAL Stacey Moultrie, BPharm , PharmD , RPh. ROCKET-AF 1 Presentation Stacey Moultrie, RPh , PharmD Candidate, 9 th Semester WPPD. Introduction: 200. Question:

E N D
ROCKET-AFology The Pharmacist look-alike Jeopardy Game Based on the ROCKET-AF TRIAL Stacey Moultrie, BPharm, PharmD, RPh
ROCKET-AF 1 PresentationStacey Moultrie, RPh, PharmD Candidate, 9th Semester WPPD
Introduction: 200 • Question: • What does Rocket AF stand for? • Answer:The RivaroxabanOnce Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonist for Prevention of Stroke and Embolism Trial in Atrial Fibrillation Back
Introduction: 400 • Question: • What two drugs were “battled it out” in this trial? • Answer • Warfarin and Rivaroxaban • 14,264 patients with NONVALVULAR atrial fibrillation were randomly assigned to rivaroxaban or warfarin Back
Introduction: 600 • Question: • What is rivaroxaban’s MOA? • Answer • It is a reversible Factor Xa inhibitor Back
Clinical relevance: 200 • Question: • True/False: Rivaroxaban requires INR monitoring. • Answer • False • Unlike warfarin which requires frequent monitoring to adjust the dose for stroke or systemic embolism to the target INR 2 to 3, rivaroxabandoes not require dose adjustment to a target INR. Back
Clinical relevance: 400 • Question: • Was this study published in a journal that was peer reviewed and credible? • Answer • Yes • It was published in the New England Journal of Medicine. • GO PATRIOTS!!! Back
Clinical relevance: 600 • Question: • True or False: Warfarin is considered the “gold standard” for prevention of stroke and systemic embolization in patients with nonvalvularAfib. • Answer: • True Back
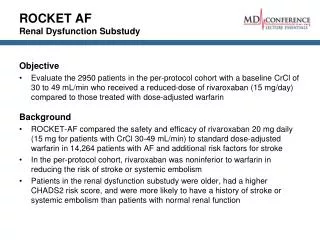
Study methods: 200 • Question: • What doses of the drugs in the study were given to the patients with normal renal function? Were the doses the same for patients with renal impairment? • Answer Patients were RANDOMLY assigned to: • rivaroxaban 20mg po daily with the evening meal + matching warfarin placebo • OR rivaroxaban 15mg po daily with the evening meal for patients with renal insufficiency/creatinine clearance of 15-50mL/min + matching warfarin placebo • OR warfarin at an adjusted dose to maintain INR of 2 to 3 (target: 2.5) + matching rivaroxaban placebo Back
Study Methods: 400 • Question: • What was the study design? • Answer • It was a randomized, multicenter double-blind (double-dummy), parallel group • Non-inferior trial Back
Study Methods: 600 • Question: • True or false: an NI design is appropriate for this study? • Answer • True • NI trials are used when placebo is inappropriate/unethical to use as a comparative agent to determine efficacy. Patients with atrial fibrillation should NOT be on a PLACEBO for prevention of stroke or systemic embolism Back
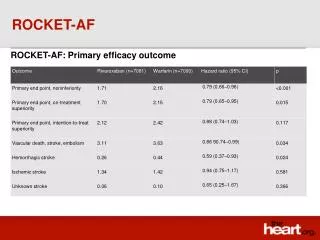
Endpoints&Results: 200 • Question: • Name the Primary and Secondary EFFICACY endpoints for this trial? • Answer • Primary: • composite of stroke and systemic embolism. • Stroke was defined as either ischemic or hemorrhagic. • Secondary: a) Composite of stroke, systemic embolism or death from CV events. b) Composite of stroke, embolism, death from CV events, OR MI. c) Individual components of composite end points. Back
Endpoints&Results: 400 • Question: • True or False: the composite of major and non-major bleeding events was the SAFETY ENDPOINT • Answer • True • Hemorrhagic/ischemic strokes or intracranial bleeds are examples of major bleeds. • Bleeding episodes that were considered non-major or minor included GI bleeds (upper, lower or rectal) or drop in hemoglobin (decreases in Hgb of less 2g per deciliter). Back
Endpoints & Results: 600 • Question: • True or false: the rivaroxaban group had a lower rate of ICH and stroke/systemic embolism than the warfarin group but a higher rate of incidence in major and non-major bleeding events. • Answer • True : Back
Limitations: 200 • Question: • True or False: an NI margin calculation is based on clinical judgment, guidelines, and other studies with similar patients? • Answer • True • NI margin depends on the size and magnitude of historical trials and is an estimated effect of how the gold standard “control” would fair against a placebo (if that was theoretically possible). • To estimate the risk ratio of warfarin versus placebo, a meta-analysis of 6 warfarin trials was used. The NI margin was determined to be 1.92; the relative risk ratio was determined to be 0.38 (95% CI 0.28-0.52).5 Back
Limitations: 400 • Question: • True or false: patients in the warfarin group were optimally managed on warfarin and were maintained on therapy with the goal INR of 2 to 3 greater than 90% of the time during this study. • Answer - False • Management of warfarin was suboptimal • INR was maintained in therapeutic range 55% of the time. The researchers claim that when the INR values were in therapeutic range, the effect of rivaroxaban did not differ. However, it has been suggested that the risks of systemic embolism or stroke is higher when the INR is below the therapeutic range of 2 to 3. Back
Limitations: 600 • Question: • True or false: The pharmaceutical company that produces rivaroxaban [Xarelto®] funded the study. • Answer • True • Johnson & Johnson and Bayer Health Care supported/funded this study. Rivaroxaban is a product of Janssen pharmaceuticals. Janssen is a pharmaceutical company of Johnson & Johnson. Many of the researchers in the study accepted consulting fees or were employees of the companies funding the study. However, there was full disclosure of conflict of interest. Back
FINAL ROCKET-AFology QUESTION: CONCLUSIONS Write down how many points you are willing to risk If you get the question right you win that many points, if you get it wrong you lose those points! Question: • Did the authors conclude that rivaroxaban was NONINFERIOR to warfarin for theprevention of stroke or systemic embolism? Answer: True. Rivaroxaban was determined to be NONINFERIOR TO WARFARIN in patients with nonvalvular atrial fibrillation. • Intracranial hemorrhage and fatal bleeding events were reduced in the rivaroxaban group but the major and non-major bleeding incidences were deemed “not clinically significantly different”. Back
References 1.) Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011 Sep 8;365(10):883-91. 2) Xarelto® (rivaroxaban) [package insert]. Janssen Pharmaceuticals; New Jersey: December 2011. 3) O'Dell KM, Igawa D, Hsin J. New Oral Anticoagulants for Atrial Fibrillation: A Review of Clinical Trials. ClinTher. 2012 Apr;34(4):894-901. 4) PL Detail-Document, Reversing Dabigatran and Rivaroxaban. Pharmacist's letter/Prescriber's Letter. September 2011. 5) ROCKET AF Study Investigators. Rivaroxaban-once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation: rationale and design of the ROCKET AF study.Am Heart J. 2010 Mar;159(3):340-347.e1. 6) Hankey GJ, Patel MR, Stevens SR, et. al (ROCKET AF Steering Committee Investigators). Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol. 2012 Apr;11(4):315-22. 7) Weitz JI, Eikelboom JW, Samama MM. New Antithrombotic Drugs: Antithrombotic Therapy for Prevention of Thrombosis: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (9th Edition). Chest. 2012 Feb;141 (2 suppl):e120S-e-151S. 8) Ahrens I, Lip GY, Peter K. What do the RE-LY, AVERROES and ROCKET-AF trials tell us for stroke prevention in atrial fibrillation? ThrombHaemost. 2011 Apr;105(4):574-8. 9) Cleland JG, Coletta AP, Buga L, et. al. Clinical trials update from the American Heart Association meeting 2010: EMPHASIS-HF, RAFT, TIM-HF, Tele-HF, ASCEND-HF, ROCKET-AF, and PROTECT. Eur J Heart Fail. 2011 Apr;13(4):460-5. 10) PL Detail-Document, Comparison of Oral Antithrombotics. Pharmacist's Letter/Prescriber's Letter. October 2011. 11) Summary of 2006 recommendations for primary and secondary prevention of stroke. Pharmacist's Letter/Prescriber's Letter 2006; 22(7):220707. 12) Rodriguez, R. Dare to Compare: Answering Healthcare Questions with Comparative Effectiveness Research (CER). Powerpoint lecture presented at Shands Hospital at the University of FL. Gainesville, FL. 8 Feb 2012.
Special Thanks • Dr. Larry Lopez • Dr. Lisa Thames • Dr. Ryan Rodriguez • Dr. Brian Kelly • Dr. Tara McCabe