Download
1 / 24
240 likes | 346 Views
The Global Epidemics of Obesity & Diabetes Paul W. Ladenson, M.D. JHI Partners Forum 2012 October 2, 2012 Baltimore. The Obesity & Diabetes Epidemics Aims. Describe relationship between overweight/obesity and diabetes from epidemiological and biological perspectives

E N D
The Global Epidemics of Obesity & Diabetes Paul W. Ladenson, M.D. JHI Partners Forum 2012 October 2, 2012 Baltimore
The Obesity & Diabetes EpidemicsAims • Describe relationship between overweight/obesity and diabetes from epidemiological and biological perspectives • Review lifestyle, public policy, medical and surgical interventions • Depict certain diabetes prevention and management programs currently offered by Johns Hopkins Medicine International
Global Diabetes Prevalences • Highest diabetes prevalences • Nauru • United Arab Emirates • Saudi Arabia • Lowest diabetes prevalences • Mongolia • Rwanda • Iceland • Death rates from diabetes and its complications are higher in low- and middle-income countries Estimated 346 million individuals affected worldwide
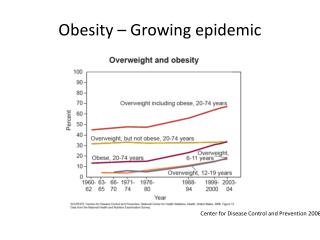
The Diabetes EpidemicPredisposing Factors • Obesity • Worldwide 500 million adults ≥20 years old obese • Highest worldwide prevalences: Nauru, Tonga, Cook Island, and Micronesia • U.S. ranked 5th highest in male obesity (44%) and 12th highest in female obesity (48%) • Body fat distribution • Race/Ethnicity • Environmental/Lifestyle
Diabetes Prevalence by Race/Ethnicity 8% Cuban, Central, South American 14% Mexican American 14% Puerto Rican American 13% 12% 8% 7% Percentage (%) Centers for Disease Control, National Diabetes Fact Sheet, 2011
The Overweight-Diabetes Relationship Varies by Race/Ethnicity • In general, Asians develop diabetes at lower BMI than Caucasians • Considerable variation among Asian groups KH, Yoon et al. Lancet. 2006; 368: 1681-1688.
Race/Ethnic Differences in Body Fat Distribution • Asian Americans have more visceral fat at similar BMI and waist size circumference compared to non-Hispanic whites
Biological Factors • Obesity and body fat distribution • Glucose metabolism and insulin resistance (compared to non-Hispanic whites) • Greater insulin resistance in minority populations independent of adiposity • Asian Americans have lower insulin secretion • Glucose metabolic features may differ in Hispanic Americans depending on country of origin
Biological Factors • Obesity and body fat distribution • Glucose metabolism and insulin resistance (compared to NHWs) • Genetics • Type 2 diabetes susceptibility loci associated in European populations also associated with increased risk in minority populations • Genome-wide association studies have identified additional diabetes-associated single-nucleotide polymorphisms in South and East Asians and in non-Hispanic blacks
Environmental/Lifestyle Factors • Assessed impact of neighborhood walkability on diabetes incidence in 214,882 recent adult Canadian immigrants • Neighborhood walkability was strong predictor of diabetes regardless of age and income, particularly among recent immigrants (RR 1.58 for men; 1.67 for women). • Poverty accentuated effect, with 3-fold greater diabetes risk in recent immigrants living in low-income/low walkability areas Diabetes Care Publish Ahead of Print, published online September 17, 2012
Environmental/Lifestyle Factors • Acculturation: “process by which immigrants adopt the attitudes, values, customs, beliefs, and behaviors of a new culture” • Socioeconomic Status: In U.S., lower income, education, and occupational status are all associated with increased diabetes risk • Health Behaviors • Diet and Exercise • Access to healthcare for obesity, diabetes, and co-morbidities (i.e., hypertension and dyslipidemia) • Effective and affordable treatments and support
Maternal Factors and Intrauterine Environment • Fetal under-nutrition and stress, maternal stress, maternal obesity modification of offspring’s gene expression and developmental biology • Low birth weight insulin resistance, diabetes, abdominal adiposity, CVD risk, elevated cortisol reactivity • Epigenetic changes in cellular gene expression: fetal adaptation to adverse intrauterine environment Kuzawa et al, Am J Hum Biol, 2009
Interventions for Diabetes Prevention & Reversal • Lifestyle modification • Public health mandates • Medication • Bariatric surgery
Diabetes InterventionsDietary and Lifestyle • Sugar-sweetened beverage consumption declined from 1.7 to nearly 0 at 1 year with intervention and remained lower at 2 years • BMI (−0.57) and weight (−1.9 kg, P=0.04) were lower at 1 year, but not at 2 years • Hispanic participants responded better with BMI and weight declines at 1 and 2 years Ebbeling et al,. New Engl J Med, ePub Sept. 25, 2012
Diabetes InterventionsDietary and Lifestyle • Assessed weight-loss interventions over 24 mos. in 415 obese patients with >1 CV risk factor: 1) Weight-loss support remotely by phone, website, and e-mail; 2) in-person group and individual sessions + remote support; or 3) self-directed weight loss. • At 24 mos, weight loss was -4.6 kg with remote support, -5.1 kg in-person support, & -0.8 kg self-directed Appel et al. N Engl J Med 2011: 365
Diabetes InterventionsBariatric Surgery Control +Guidance Surgery Carlsson et al. N Engl J Med 2012: 367:695-704
Diabetes InterventionsThe Diabetes Prevention Program • 3,234 overweight or obese adults with impaired glucose tolerance (prediabetes) assigned to receive: 1) lifestyle intervention aimed at modest weight loss through diet and exercise, 2) metformin treatment, or 3) placebo. • Lifestyle intervention and metformin reduced conversion to diabetes by 58% and 31%, respectively, over 3 years. • Lifestyle intervention was effective in both sexes, across racial and ethnic groups, and with genetic predisposition • Lifestyle intervention worked best in participants 60 or older, a group in which metformin did not benefit. • Metformin worked well among younger participants, esp. women with history of gestational diabetes. Knowler et al. N Engl J Med 2002: 346:393-403
JHI Diabetes Programs Aims • Build professional capacity & expertise • Characterize state of diabetes patients and their care • Use data to improve quality of care delivery • Implement point-of-care laboratory technologies • Develop diabetic retinopathy screening program • Heighten public awareness & prevention
Johns Hopkins Diabetes International Programs • The Johns Hopkins Diabetes Guide (Trinidad & Tobago, Kuwait, & India) • Trinidad & Tobago Olympic Committee collaboration for diabetes risk detection and prevention in children • Diabetes database and care performance monitoring system (Trinidad)
TTHSI Diabetes Outreach Program Diabetes Care Performance Improvement
TTHSI Diabetes Outreach Program Diabetes Care Performance Improvement • Sustainable Continuous Quality Improvement based on data collected and dashboard reporting Deficit Identified in Dashboard Data Remedy Proposed,Considered &Implemented Impact of InterventionAssessed
Johns Hopkins Diabetes International Programs • Health Professional education & empowerment • Academy of Diabetes Clinicians of Trinidad & Tobago • Nurse diabetes education and empowerment (Kuwait and Trinidad) • Medical second opinion service (Kuwait) • Inpatient diabetes management service • Johns Hopkins Diabetes Center affiliations
Obesity & Diabetes International Solutions • Epidemics of chronic metabolic disorders represent threats to health and challenges for healthcare systems • Research is revealing the biological and environmental factors responsible • Solutions are being developed and implemented—from lifestyle to medication and surgery • JHI currently offers a set of interventions and experience implementing them internationally