Download
1 / 1
10 likes | 188 Views
Sweet syndrome: Neutrophilic Dermatitis, A Marker of Systemic Disease. Lisa Johnson, D.O. PGY II & Christopher Colbert, D.O. Department of Emergency Medicine, Franciscan St. James Health, Olympia Fields, IL. Abstract. Figures. Discussion. Historical. Past Medical History: Patient denies

E N D
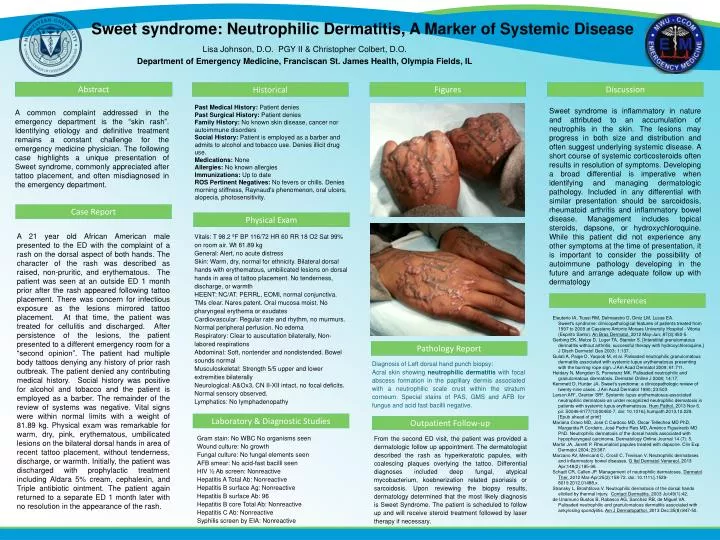
Sweet syndrome: Neutrophilic Dermatitis, A Marker of Systemic Disease Lisa Johnson, D.O. PGY II & Christopher Colbert, D.O. Department of Emergency Medicine, Franciscan St. James Health, Olympia Fields, IL Abstract Figures Discussion Historical Past Medical History: Patient denies Past Surgical History: Patient denies Family History: No known skin disease, cancer nor autoimmune disorders Social History: Patient is employed as a barber and admits to alcohol and tobacco use. Denies illicit drug use. Medications: None Allergies: No known allergies Immunizations: Up to date ROS Pertinent Negatives: No fevers or chills. Denies morning stiffness, Raynaud's phenomenon, oral ulcers, alopecia, photosensitivity. • Sweet syndrome is inflammatory in nature and attributed to an accumulation of neutrophils in the skin. The lesions may progress in both size and distribution and often suggest underlying systemic disease. A short course of systemic corticosteroids often results in resolution of symptoms. Developing a broad differential is imperative when identifying and managing dermatologic pathology. Included in any differential with similar presentation should be sarcoidosis, rheumatoid arthritis and inflammatory bowel disease. Management includes topical steroids, dapsone, or hydroxychloroquine. While this patient did not experience any other symptoms at the time of presentation, it is important to consider the possibility of autoimmune pathology developing in the future and arrange adequate follow up with dermatology A common complaint addressed in the emergency department is the “skin rash”. Identifying etiology and definitive treatment remains a constant challenge for the emergency medicine physician. The following case highlights a unique presentation of Sweet syndrome, commonly appreciated after tattoo placement, and often misdiagnosed in the emergency department. Case Report Physical Exam A 21 year old African American male presented to the ED with the complaint of a rash on the dorsal aspect of both hands. The character of the rash was described as raised, non-pruritic, and erythematous. The patient was seen at an outside ED 1 month prior after the rash appeared following tattoo placement. There was concern for infectious exposure as the lesions mirrored tattoo placement. At that time, the patient was treated for cellulitis and discharged. After persistence of the lesions, the patient presented to a different emergency room for a “second opinion”. The patient had multiple body tattoos denying any history of prior rash outbreak. The patient denied any contributing medical history. Social history was positive for alcohol and tobacco and the patient is employed as a barber. The remainder of the review of systems was negative. Vital signs were within normal limits with a weight of 81.89 kg. Physical exam was remarkable for warm, dry, pink, erythematous, umbilicated lesions on the bilateral dorsal hands in area of recent tattoo placement, without tenderness, discharge, or warmth. Initially, the patient was discharged with prophylactic treatment including Aldara 5% cream, cephalexin, and Triple antibiotic ointment. The patient again returned to a separate ED 1 month later with no resolution in the appearance of the rash. Vitals: T 98.2 ºF BP 116/72 HR 60 RR 18 O2 Sat 99% on room air. Wt 81.89 kg General: Alert, no acute distress Skin: Warm, dry, normal for ethnicity. Bilateral dorsal hands with erythematous, umbilicated lesions on dorsal hands in area of tattoo placement. No tenderness, discharge, or warmth HEENT: NC/AT. PERRL, EOMI, normal conjunctiva. TMs clear. Nares patent. Oral mucosa moist. No pharyngeal erythema or exudates Cardiovascular: Regular rate and rhythm, no murmurs. Normal peripheral perfusion. No edema Respiratory: Clear to auscultation bilaterally, Non-labored respirations Abdominal: Soft, nontender and nondistended. Bowel sounds normal Musculoskeletal: Strength 5/5 upper and lower extremities bilaterally Neurological: A&Ox3, CN II-XII intact, no focal deficits. Normal sensory observed. Lymphatics: No lymphadenopathy References • Eleuterio IA, Tiussi RM, Delmaestro D, Diniz LM, Lucas EA. Sweet's syndrome: clinicopathological features of patients treated from 1997 to 2009 at Cassiano Antonio Moraes University Hospital - Vitoria (Espirito Santo). An Bras Dermatol. 2012 May-Jun; 87(3):450-5. • Gerbing EK, Metze D, Luger TA, Stander S. [Interstitial granulomatous dermatitis without arthritis: successful therapy with hydroxychloroquine.] J Dtsch Dermatol Ges 2003; 1:137. • Gulati A, Paige D, Yaqoob M, et al. Palisaded neutrophilic granulomatous dermatitis associated with systemic lupus erythematosus presenting with the burning rope sign. J Am Acad Dermatol 2009; 61:711. • Heidary N, Mengden S, Pomeranz MK. Palisaded neutrophilic and granulomatous dermatosis. Dermatol Online J 2008; 14:17. • Kemmett D, Hunter JA. Sweet’s syndrome: a clinicopathologic review of twenty-nine cases. J Am Acad Dermatol 1990; 23:503 • Larson AR1, Granter SR2. Systemic lupus erythematosus-associated neutrophilic dermatosis-an under recognized neutrophilic dermatosis in patients with systemic lupus erythematosus. Hum Pathol. 2013 Nov 6. pii: S0046-8177(13)00460-7. doi: 10.1016/j.humpath.2013.10.029. [Epub ahead of print] • Mariana Cravo MD, José C Cardoso MD, Oscar Tellechea MD PhD, Margarida R Cordeiro, José Pedro Reis MD, Américo Figueiredo MD PhD. Neutrophilic dermatosis of the dorsal hands associated with hypopharyngeal carcinoma. Dermatology Online Journal 14 (7): 5. • Martin JA, Jarrett P. Rheumatoid papules treated with dapsone. Clin Exp Dermatol 2004; 29:387. • Marzano AV, Menicanti C, Crosti C, Trevisan V. Neutrophilic dermatoses and inflammatory bowel diseases. G Ital Dermatol Venereol. 2013 Apr;148(2):185-96. • Schadt CR, Callen JP. Management of neutrophilic dermatoses. Dermatol Ther. 2012 Mar-Apr;25(2):158-72. doi: 10.1111/j.1529-8019.2012.01488.x. • Stransky L, Broshtilova V. Neutrophilic dermatosis of the dorsal hands elicited by thermal injury. Contact Dermatitis. 2003 Jul;49(1):42. • de Unamuno Bustos B, Rabasco AG, Sanchez RB, de Miguel VA. Palisaded neutrophilic and granulomatous dermatitis associated with ankylosing spondylitis. Am J Dermatopathol. 2013 Dec;35(8):847-50. Pathology Report Diagnosis of Left dorsal hand punch biopsy: Acral skin showing neutrophilic dermatitis with focal abscess formation in the papillary dermis associated with a neutrophilic scale crust within the stratum corneum. Special stains of PAS, GMS and AFB for fungus and acid fast bacilli negative. Laboratory & Diagnostic Studies Outpatient Follow-up Gram stain: No WBC No organisms seen Wound culture: No growth Fungal culture: No fungal elements seen AFB smear: No acid-fast bacilli seen HIV ½ Ab screen: Nonreactive Hepatitis A Total Ab: Nonreactive Hepatitis B surface Ag: NonreactiveHepatitis B surface Ab: 96 Hepatitis B core Total Ab: Nonreactive Hepatitis C Ab: Nonreactive Syphilis screen by EIA: Nonreactive From the second ED visit, the patient was provided a dermatologic follow up appointment. The dermatologist described the rash as hyperkeratotic papules, with coalescing plaques overlying the tattoo. Differential diagnoses included deep fungal, atypical mycobacterium, koebnerization related psoriasis or sarcoidosis. Upon reviewing the biopsy results, dermatology determined that the most likely diagnosis is Sweet Syndrome. The patient is scheduled to follow up and will receive steroid treatment followed by laser therapy if necessary.