Download
1 / 57
1.09k likes | 2.67k Views
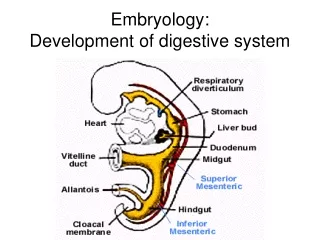
DEVELOPMENT OF DIGESTIVE SYSTEM. BODY FOLDING. The longitudinal and transverse folding of the embryo is occured in the 3rd and 4th weeks This event converts the flat trilaminar embryonic disc into a trilaminar , elongated cylinder .

E N D
BODY FOLDING • The longitudinaland transverse folding of the embryo is occured in the 3rd and 4th weeks • This event convertsthe flat trilaminar embryonic disc into a trilaminar, elongated cylinder. • Cranio-caudal body folding is formedendodermal pocket. • Thelateral body folds meet in the ventral midline and fuse to generate the elongated body cylinder. • By the time body folding is nearly complete, the gut tube consists of cranial and caudal blind-ending tubes, • A blind ending tubes dvides three part; foregut, midgut, and hindgut. • Acentralpart of gut (midgut) still opens ventrally to the yolk sac. • Cranially, the foregut terminates at the oropharyngeal membrane (or buccopharyngeal membrane); • Caudally, the hindgut terminates at the cloacal membrane. • The vitelline duct and yolk sac are eventually incorporated into the umbilical cord.
BODY FOLDING • The outer layer is the ectoderm (the future skin). • Ectoderm covers the outer surface of the embryo except in the umbilical region. • The innermost layer is the endodermalprimary gut tube. • Separating these two layers is a layer of mesoderm that contains the coelom. • During the process of lateral body folding, the endodermal lining of the gut tube becomes surrounded by cells derived from lateral plate splanchnic mesoderm. • This mesoderm condenses and differentiates into the lamina propria, submucosa, muscular walls, vascular elements, and connective tissue of the gastrointestinal tract. • Some genes involved in body folding such asGata4, Sox17, and Furin/Spc1.
Dorsal Mesentery Initially Suspends Abdominal Gut Tube • When the coelom first forms, the gut is broadly attached to the dorsal body wall by mesoderm. • The mesenchyme within cranial region of attachment gradually spreads during the 4th week from cranial to caudal direction. • As a result, thin, bilayered mesenchyme is formed a dorsal mesentery. • The dorsal mesentery suspends the abdominal viscera in the coelomic cavity. • A coelomic cavity will later become the peritoneal cavity, • The abdominal vicrera are referred to as intraperitoneal viscera.
RETROPERITONEAL ORGANS • In contrast to some of the visceral organs develop within the body wall. • They are separated from the coelom by a covering of serous membrane. • These organs are said to be retroperitoneal(outside the coelomic cavity). • The kidneys the bladder are retroperitoneal. • Kidneys develops in the posterior body wall but bladdergrows anterior body wall. • The gut tube are initially suspended by mesentery,later become fused to the body wall. • Thus, some organs stays out of thecoelomic cavity. • These organs are called secondarily retroperitonealsuch as the ascending and descending colon, duodenum, and pancreas,.
VENTRAL MESENTERY • At the end of the 4th week, almost the entire abdominal gut tube is suspended by the dorsal mesentery. • Thera is one exception; the developing stomach. • During lateral folding, the coelomic cavities coalesce to form a single, continuous peritoneal cavity. • In the stomach region, the gut tube remains connected to the ventral body wall by the thick septum transversum. • By the 5th week, the caudal portion of the septum transversum formsthe ventral mesentery. • Ventral mesentery connectsthe stomach and developing liver.
Three Regions of Primitive Gut • The boundaries of the foregut, midgut, and hindgut correspond to the territories of the three supplying arteries. • The gut tube and its derivatives are vascularized by unpairedventral branches of the descending aorta. • Three arteries serve the remainder of the gut tube: • The celiac trunk, which supplies the abdominal foregut (the abdominal esophagus, stomach, and cranial half of the duodenum and its derivatives); The superior mesenteric trunk, which supplies the midgut; • The inferior mesenteric artery, which supplies the hindgut.
FORMATION OF STOMACH • The stomach first becomes apparent during the early part of the 4th week, in place of the caudal foregut. • On about day 26, the thoracic foregut begins to elongate rapidly. • Over the next 2 days, the presumptive stomach is removedfrom the lung buds. • Developing stomach expands into a fusiform (Latin, "spindle-shaped") structure. • During the 5th week, the dorsal wall of the stomach grows faster than the ventral wall, resulting in the formation of the greater curvature of the stomach. • Synchronously, deformation of the ventral stomach wall forms the lesser curvature of the stomach. • By the end of the 7th week, the continual differential expansion of the superior part of the greater curvature results in the formation of the fundus and cardiac incisure.
ROTATION OF STOMACH • During the 7th and 8th weeks, the developing stomach undergoes a 90-degree rotation around its craniocaudal axis • Sothat the greater curvature lies to the left and the lesser curvature lies to the right. • Differantial thinning of the right side of the dorsal mesogastriumis believed to play a role in this rotation. • The stomach also rotates slightly around a ventrodorsal axis so that the greater curvature faces slightly caudally, and the lesser curvature slightly cranially.
ROTATION OF STOMACH • The rotations of the stomach bend the presumptive duodenum. • Duedonum displace to the right until it lies against the dorsal body wall, • Duedonum adheres dorsal body wall and becomes secondarily retroperitoneal. • The rotation of the stomach and the fusion of the duodenum create an niche dorsal to the stomach called the lesser sac of the peritoneal cavity. • The rest of the peritoneal cavity is now called the greater sac.
ROTATION OF STOMACH • The lesser sac enlarges because of progressive expansion of the dorsal mesogastrium. • The resulting large, suspended fold of mesogastrium, called the greater omentum, • Greate omentum hangs from the dorsal body wall and the greater curvature of the stomach. • The portion of the lesser sac directly dorsal to the stomach is now called the upper recess of the lesser sac. • The cavity within the greater omentum is called the lower recess of thelesser sac. • The lower recess is obliterated during fetal life as the anterior and posterior folds of the greater omentum.
Development of Liver and Gallbladder • On about day 22, the hepatic plateforms on the ventral side of the duodenum. • Over the next few days, cells in this plate proliferate and form the hepatic diverticulum, • The cells of hepatic plategrows into mesenchymalcells. • The cells of hepatic plate will give rise to the inferior region of the septum transversum. • The hepatic diverticulum gives rise to branching cords of hepatoblasts(the liver primordial cells). • Hepatoblasts are cytologicallyundifferentiated at this stage. • Under the influence of Notch signaling and other regulatory proteins,hepatoblastsbecome hepatocytes(parenchyma), bile canaliculiof the liver, or hepatic ducts. • In contrast, the mesoblasticsupporting stromadevelops from the septum transversum and splanchnic mesoderm originating near the stomach. • Origin of endothelial precursor cells are unknown.
LIVER AS HEMATOPOETIC ORGANS The liver is a major early hematopoietic organ of the embryo. Hematopoietic stem cells originating from the yolk sac. These stem cells colonize the embryonic liver, These colonies expand their numbers, and spread before populating other hematopoietic organs. Throughout embryonic and fetal development, hepatocytes proliferate (mainly mediated by autocrine mechanisms). This proliferation gradually slows and is arrested with postnatal development.
DEVELOPMENT OF BILIARY TRACT • By day 26, a distinct endodermal thickening forms to the base of the hepatic diverticulum • This buds appear into the ventral mesentery. • This cystic diverticulum will form the gallbladder and cystic duct. • Thecystic diverticulum proliferate and form the common bile duct. • As a result, the developing cystic duct is carried away from the duodenum.
DEVELOPMENT OF PANCREAS • On day 26, another duodenal bud begins to grow into the dorsal mesentery just opposite the hepatic diverticulum. • This endodermal diverticulum is the dorsal pancreatic bud. • Over the next few days, as the dorsal pancreatic bud elongates into the dorsal mesentery, • The ventral pancreatic bud develops into the ventral mesentery just caudal to the developing gallbladder. • By day 32, the main duct of the ventral pancreatic bud becomes. • Main duct of the ventral pancreatic bud is connected to the proximal end of the common bile duct.
DEVELOPMENT OF PANCREAS PARENCHYMA CELLS • The pancreatic endoderm thickens, forming a multilayered solid bud within the duodenal portion of the gastrointestinal tract. • This solid bud continues to proliferate into the closely apposed mesoderm. • The branching of this bud occurs differently from the classic branching of other organs. • The epithelium expandsand folds in this way epithelial clusters form. • Then intraepithelial microlumens appaers in the epithelial clusters. • Several microlumens coalesce to generate continuous lumens. • Forming an epithelial tree provides draining exocrine products into the duodenum.
DEVELOPMENT OF PANCREAS PARENCHYMA CELLS Thepancreatic exocrine cells produce digestive enzymes, the Thepancreatic ductal cells transport the digestive enzymes, The pancreatic endocrine cells in the islets of Langerhans produce insulin, glucagon, and somatostatin. All differentiate from the endoderm of the pancreatic buds. Theendocrine cell lineage proliferates within the endodermal epithelium. These cells delaminate and subsequently aggregate into islets. They continue to proliferate throughout the embryonic period.
FUSION OF PANCREATIC BUDS • The common bile duct and ventral pancreatic bud are branching, proliferating, and differentiating. • The mouth of the common bile duct and ventral pancreatic bud migrate posteriorly around the duodenum . • By the early 6th week, the ventral and dorsal pancreatic buds lie adjacent in the plane of the dorsal mesentery. • Late in the 6th week, the two pancreatic buds fuse to form the definitive pancreas. • The dorsal pancreatic bud gives rise to the head, body, and tail of the pancreas, • The ventral pancreatic bud gives rise to the hook-like uncinate process. • Like the duodenum, the pancreas fuses to the dorsal body wall and becomes secondarily retroperitoneal.
DEVELOPMENT OF PANCREATIC DUCTS • When the ventral and dorsal pancreatic buds fuse, their ductal systems also become interconnected. • The duct connecting the dorsal bud to the duodenum usually degenerates, now called the main pancreatic duct. • The main pancreatic duct and the common bile duct meet and empty their secretions into the duodenum at the major duodenal papilla or ampulla of Vater. • In some individuals, the dorsal pancreatic duct persists as an accessory pancreatic duct that empties into the duodenum at a minor duodenal papilla.
IN THE CLINIC: ABNORMAL FORMATION AND ROTATION OF VENTRAL PANCREAS • Occasionally, the pancreas forms a complete ring encircling the duodenum, a condition known as annular pancreas. • The ventral pancreas may consist of two lobes. • If the lobes migrate around the duodenum in opposite directions to fuse with the dorsal pancreatic bud, an annular pancreas is formed. • An annular pancreas compresses the duodenum. • This situation may cause gastrointestinal obstruction (duodenal stenosis).
IN THE CLINIC: HYPERINSULINISM The number of islet cells develops in the pancreas during fetal life Some factors can be influenced intrauterine growth restriction (IUGR) such as vascular insufficiency, maternal diabetes, and fetal malnutrition. In utero islet cells respond to elevated blood glucose levels with compensatory hyperplasia. This fetal maladaptation is frequently seen in neonates born to diabetic mothers. Compensatory hyperplasia can occur locally or diffusely throughout the pancreas. This circumstance is called congenital hyperinsulinism. Hyperinsulinemia causes in decrease of blood glucose levels(i.e., hypoglycemia). Hyperinsulinemia is typically treated by diazoxide therapy. The hyperinsulinemia is resolved by partial or near-total pancreatectomy.
IN THE CLINIC: REGULATION OF NUMBER OF ISLET CELLS Before birth, islet cells are generated through the proliferation and differentiation of pancreatic progenitor cells. The number of islets is maintained proper glucose levels during embryonic and fetal period. The capacity to generate more islet cells after birth is greatly reduced. Theislet cell population can still increase, very slowly and with limited capacity, at least until adolescence. If human adult pancreatic beta cells share this proliferative capacity, new therapeutic strategies for humantype I diabetes could be developed.
DEVELOPMENT OF SPLEEN • As the dorsal mesogastrium of the lesser sac begins its expansive growth at the end of the 4th week. • Amesenchymal condensation develops in it near the body wall. • This condensation differentiates during the 5th week to form the spleen. • Smaller splenic condensations is called accessory spleens • The accessory spleen may develop near the hilum of the primary spleen. • The spleen is a mesodermal derivative.
DEVELOPMENT OF SPLEEN • The rotation of the stomach • The growth of the dorsal mesogastrium • Result in, spleen translocate to the left side of the abdominal cavity. • The renal-splenic ligament establishes between the spleen and the left kidney. • The gastrosplenic ligamentoccursbetween the spleen and the stomach in the dorsal mesentery.
Development of Spleen • The spleen initially functions as a hematopoietic organ. • Thepreliminary stage (until 14 weeks);the spleen is strictly hematopoietic. • The transformation stage(from15 to 18 weeks);the organ develops its characteristic lobular architecture. • The stage of lymphoid colonization: • T-lymphocyte precursor cells begin to enter the spleen. • B-cell precursors arrive and form the B-cell regions at starting of 23 weeks.
Derivatives of Ventral Mesentery • The caudal portion of the septum transversum and the ventral mesentery are modified and formeda number of membranous structures. • The liver and the membranes attach to the stomach and to the ventral body wall. • By the 6th week, the enlarging liver makes contact with the septum transversum . • The portion of the ventral mesentery coversthe liver and begins to seperate. • The central tendon of the diaphragm forms from the septum transversum. • At the cranial end, the liver tissue makes direct contact with the central tendon of the diaphragm. • This zone becomes the bare area of the liver. • The bare area like a crown, it is called the coronary ligament.
DEVELOPMENT OF THE GREATER OMENTUM • The narrow sickle-shaped flap of ventral mesentery differentiates into the membranous falciformligament. • The lesser omentum developsbetween the liver and the stomach. • This part of ventral mesentery thins out to form a translucent membrane. • The hepatoduodenalligament providesconnecting the liver to the duodenum from the caudal border of the lesser omentum. • The hepatoduodenal ligament contains the portal vein, the proper hepatic artery and its branches, and the hepatic, cystic, and common bile ducts. • Thehepatogastricligamentforms between the liver and the stomach.
EPIPLOIC FOREMEN OF WINSLOW • The lesser omentum rotates from a sagittal into a coronal (frontal) plane, when the stomach rotates to the left. • This repositioning reduces the communication between the greater and lesser sacs of the peritoneal cavity. • A narrow canal lying just posterior to the lesser omentum. • This canal is called the epiploic foramen of Winslow.
DEVELOPMENT of PRIMARY INTESTINAL LOOP • By the 5th week, the presumptive ileum and the presumptive colon can be distinguished at the abdominal region. • A cecalprimordiumpresents between the ileum and colon. • The ileum elongatesmuch more rapidly than the abdominal cavity. • Two limbs compose to dorsoventralhairpin fold and it is called the primary intestinal loop • The cranial limb of this loop will give rise to most of the ileum; • Thecaudal limb will become the ascending colon and transverse colon. • At its apex, the primary intestinal loop is attached to the umbilicus by the vitelline duct, • The superior mesenteric artery runs down the long axis of the loop.
DEVELOPMENT of PRIMARY INTESTINAL LOOP • By the early 6th week, the midgut elongation continues. • Mid gut elongation and the pressure of other abdominal organs growth are two force. • Resulting from combined effect, primary intestinal loop herniatesinto the umbilicus. • Herniate intestinal loop rotatesaround the dorsoventral axis by 90 degrees counterclockwise. • Thus, the cranial limb moves caudally and to the embryo's right, • The caudal limb moves cranially and to the embryo's left. • This rotation is complete by the early 8th week.
RETRACTION of PRIMARY INTESTINAL LOOP • The lengthening jejunum and ileum arethrown into a series of folds called the jejunal-ileal loops • The expanding cecum sprouts a wormlike vermiform appendix. • During the 10th week, the midgut retracts into the abdomen and rotates an additional 180 degrees. • Thus, the retracting colon has traveled a 270-degree circuit.
RETRACTION of PRIMARY INTESTINAL LOOP • The colon is locate to the posterior wall of the abdominal cavity. • The cecum consequently rotates to a position just inferior to the liver in the region of the right iliac crest. • The intestines have completely returned to the abdominal cavity by the 11th week.
DEVELOPMENT of PRIMARY INTESTINAL LOOP • After the large intestine returns to the abdominal cavity, the ascending colon and descending colon contact with the dorsal body wall. • They become secondarily retroperitoneal.
IN THE CLINIC: ABNORMAL ROTATION AND FIXATION OF MIDGUT The normal-handed asymmetry of the midgut is based on a relatively complexseries of rotations and fixations. Not surprisingly, errors in one or more of these steps lead to a varied spectrum of anomalies in humans. The presence of a rotational abnormality is usually signaled during infancy or childhood by the sudden onset of acute abdominal pain. Other symptoms and signs arevomiting, or gastrointestinal bleeding, or by intermittent vomiting or failure to thrive (growth retardation). Occasionally, such an abnormality remains clinically silent until adulthood. Definitive diagnosis involves barium swallow or barium enema in conjunction with X-rays.
ROTATIONAL DEFECT OF MIDGUTNONROTATION OF THE MIDGUT • The primary intestinal loop fails to undergo the normal 180-degree counterclockwise rotation. • Midgutis retracted into the abdominal cavity. • The anomaly called nonrotation of the midgut. • The earlier 90-degree rotation may occur normally. • The result of this error: • The original cranial limb of the primary intestinal loop ends up on the right side of the body, • The original caudal limb of the primary intestinal loop ends up on the left side of the body. • Therefore, this condition is sometimes called left-sided colon.
REVERSE ROTATION OF THE MIDGUT • The primary intestinal loop undergoes the initial 90-degree counterclockwise rotation normally. • Butthe second 180-degree rotation occurs clockwise. • Sothe net rotation of the midgut is 90 degrees clockwise. • This rotation brings the regions of the midgut and hindgut into their normal spatial relationships. • Important Exception: the duodenum lies ventral to the transverse colon instead of dorsal to it. • The duodenum thus does not become secondarily retroperitoneal.
MIXED ROTATION (MALROTATION) OF THE MIDGUT • Only the cephalic limb of the primary intestinal loop undergoes the initial 90-degree rotation. • Only the caudal limb undergoes the later 180-degree rotation. • The result of this: • The distal end of the duodenum becomes fixed on the right side of the abdominal cavity, • The cecumbecomes fixed near the midline just inferior to the pylorus of the stomach. • This abnormal position of the cecum may cause the duodenum to be enclosed by a band. • The small intestines is tethered on the right. • This state increases the risk of an intestinal obstruction.
VOLVULUS OF INTESTINE • Most cases of intestinal obstruction are caused by abnormal rotation or fixation of the midgut. • Intestinal volvulus is defined as a complete twisting of a loop of intestine around its mesenteric attachment site. • Such freely suspended coils are prone to torsion or volvulus. • Volvuluscauses symptoms by two mechanisms: • One is bowel obstruction. • The other is ischemia (loss of blood flow) to the affected portion of intestine. • Obstructive symptoms: • «Bilious vomiting»is a common symptom of intestinal volvulus. • Acute abdominal pain • Ischemic symptoms: • Gastrointestinalbleeding. • Volvulus must be treated surgically.
DEFECTS OF THE UMBILICUS AND ANTERIOR ABDOMINAL WALL: MECKEL’S DIVERTICULUM • The vitelline duct normally regresses between the 5th and 8th weeks. • Inabout 2% of live-born infants vitelline duct persistsas a remnant of variable length and location. • It is observed as a 1- to 5-cm intestinal diverticulum projecting from the antimesentericwall. • In other cases, part of the vitelline duct within the abdominal wall persists, • Anopen omphalomesenteric fistula, • Anomphalomesenteric cyst (or enterocyst), • Anomphalomesentericligament (or fibrous band). • Meckel'sdiverticulum is about twice as common in males as in females.
Meckel's Diverticulum • Most cases of Meckel's diverticulum are asymptomatic. • However, it is estimated that 15% to 35% of individuals who have Meckel's diverticulum develop symptoms. • These symptoms: Intestinal obstruction, gastrointestinal bleeding, or peritonitis (before 10 years of age). • Meckel'sdiverticulum complications can manifest as a consequence of bowel obstruction. Symptoms may closely mimic appendicitis, involving periumbilical pain that later localizes to the right lower quadrant. • Up to 60% of Meckel's diverticula include abnormal tissue, usually pancreatic or gastric. • Patients may develop bleeding,ulceration of the gut. • Mortality in untreated cases is estimated to be 2.5% to 15%.
RULE OF TWOS • The facts about Meckel's diverticulum can be remembered using the "rule of twos": • Itoccurs in 2% of the population, • Itis 2 times more common in males, • 2% of individuals with Meckel's diverticulum have medical symptoms, • Ussually it is appear2 years of age, • it is usually present 2 feet proximal to the terminal ileum, • It is usually 2 inches long, • Itcontains 2 types of abnormal lining.
Umbilical Hernia, Omphalocele, and Gastroschisis • The terms used to describe defects of the anterior abdominal wall in which the abdominal contents protrude. • Here, they are divided into three groups: • Umblical hernia, • Ompholocele, • Gastroschisis. • An umbilical hernia consists of a small protrusion of bowel through the umbilical ring, which is covered by skin. • It is often more apparent when the infant cries. • More than 95% of umbilical hernias close spontaneously by 5 years of age.
Omphalocele • Omphaloceleinvolves herniation of bowel or other viscera through the umbilical ring, • Ompholocele is covered by a thin avascular membrane that may rupture. • Omphaloceleoccurs in about 2.5 of 10,000 births, • It is often associated with chromosome abnormalities or other malformation syndromes. • Several possible explanations for omphalocele exist. • One possibility:The herniated bowel does not fully retract into the abdominal cavity during the 10th week. • Another possibility:Lateral body folding and fusion fails to occur properly during the 4th to the 8th weeks. • A third possibility:Incompletemigration and differentiation may occur the mesoderm. • In this results, the connective tissue of the skin and hypaxial musculature can not normally forms.
Gastroschisis • Gastroschisisis a defect of the anterior abdominal wall. • Bowel protrudes without a covering sac between the developing rectus muscles. • In gastroschisis, the umbilical ring closes normally. • The cause of gastroschisis, like that of omphalocele. • Gastroschisisdiffers from omphalocele in being less often associated with other abnormalities, • Ithas not been correlated with chromosomal anomalies. • The incidence of this defect is about 1 in 10,000 births. • Other defects of the anterior body wall include ectopiacordis, isolated protrusion of the heart through the body wall, • A group of five defects calledpentalogyof Cantrell (supraumbilical abdominal wall defect, diaphragmatic hernia, pericardial defect, sternal cleft, and intracardiac anomaly).
Cytodifferentiation of Endodermal Epithelium of Gut • The gastrointestinal tract is composed of • Theendoderm forming the epithelial lining of the lumen, • Thesplanchnic mesoderm forming the smooth muscle and connective tissue tunics, • Theectoderm. • Early in development, much of the endodermal lining of the gastrointestinal tract remains uniform in morphology until epithelial-mesenchymal interactions. • Many of the major morphologic changes and cytodifferentiation events occur during the midgestation (fetal) period.
Endodermal Epithelium of Gut • Initially, the gastrointestinal epithelium is pseudostratified but is converted into a simple columnar epithelium. • Early in the 2nd month, the lumen of the gastrointestinal tract is temporarily occluded. • Over the next two weeks vacuoles develop within the base of the thickened epithelial layer and coalesce until the gut tube is fullyrecanalized. • Mesodermalexpansions project into the region of vacuolization. • Epithelium and mesodermal expansions form the villi of the intestines. • In the intestines, formation of villi is accompanied by endodermal invagination into the mesoderm, forming crypts. • In the stomach, villi do not form • Theendoderm does invaginate into the mesoderm, forming pits (future gastric glands). • Finally, in the 9th week, the definitive mucosal epithelium differentiates from the endodermal lining of the regenerated gut lumen.
Development of Outer Intestinal Wall and Its Innervation • The gut tube consists of an endodermally derived epithelium covered by splanchnopleuric mesoderm. • The mesodermal layer develops into multiple layers including the lamina propria, muscularis mucosa, submucosa, and circular and longitudinal muscular layers. • Innervation of these layers is via the enteric nervous system composed collectively of sympathetic and parasympathetic components. • The enteric nervous system eventually becomes arranged in two general layers, the inner Meissner's plexus(between submucosa and smooth muscle layer) and Auerbach's plexus (on the outer portion of the smooth muscle tunic).
IN THE CLINIC: HIRSCHSPRUNG DISEASE • Disorders of enteric nervous system in humans can be divided into two major groups: • those characterized by an abnormal number of ganglia (Hirschsprung), • those characterized by abnormal neuronal differentiation (intestinal neuronal dysplasia). • In Hirschsprung disease (1 in 5000 live births; also known ascongenital aganglionicmegacolon), • There is a complete or partial obstruction of intestine due to total absence of both myentericand submucosa ganglia. • This leads to abnormal dilation or distention of a variable length of the colon, and increased wall thickness due to muscular hypertrophy in the intestine proximal to the aganglionic segment. • The enlarged bowel (i.e., megacolon) in patients with Hirschsprung disease is essentially a secondary symptom caused by the obstruction and lack of peristalsis in the colon segment distal to the dilation. • Removal of the constricted distal segment remains the only effective treatment for the disease.
IN THE CLINIC: HIRSCHSPRUNG DISEASE The first sign of Hirschsprung disease is usually a delay in the passage of meconium (usually meconium is passed within 48 hours). This may be accompanied by other symptoms such as constipation, vomiting, abdominal pain, and distention. These patients are at risk for life-threatening complications such as intestinal infection (enterocolitis) or rupture of the cecum. Most individuals with Hirschsprung disease are diagnosed during their first year of life. Barium enema examinations show the nonperistaltic segment usually involves the sigmoid colon and rectum. Diagnosis of Hirschsprung disease is made by suction biopsy of the rectal mucosa, with histopathology demonstrating an absence of enteric ganglia.