Download
1 / 23
240 likes | 420 Views
Type 1 vs. Type 2 Diabetes…. What are we Treating?. Ida Reighard RN, CDE St James Healthcare 723-2960/ida.reighard@sjh-mt.org. Objectives:. At the end of this continuing medical education event, participants should be able to: Name 2 differences between Type 1 and Type 2 Diabetes

E N D
Type 1 vs. Type 2 Diabetes….What are we Treating? Ida Reighard RN, CDE St James Healthcare 723-2960/ida.reighard@sjh-mt.org
Objectives: At the end of this continuing medical education event, participants should be able to: • Name 2 differences between Type 1 and Type 2 Diabetes • Name 2 psychosocial concerns related to Type 1 and Type 2 Diabetes • Identify pharmaceutical therapies for Type 1 and Type 2 Diabetes
Disclosures • Criteria for Successful Completion: Attendance for at least 80% of the educational event. • Disclosure of presenter: Ida Reighard RN, CDE has nothing to disclose. • Disclosures of those in a position to control educational content: Phil Dean RN – Clinical Nurse Educator has nothing to disclose.
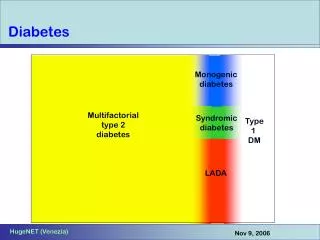
You need to know “what” you’re treating: • Pills never worked • Insulin added quickly • Ketones in urine or DKA • Type 1 • Absolute Insulin Deficiency • Treated with insulin • Average age 14-40 at onset • Typically lean body • Genetically set up • <10% of people with diabetes
What is Type 2 Diabetes? • Defined by a Complex metabolic disorder…… (Both Insulin resistance and deficiency) Include the social, behavioral and environmental risk factors unmasking the effects of genetic susceptibility. i.e. it’s complex
You need to know “what” you’re treating: • Type 2 • Relative Insulin Deficiency • Insulin Resistance • Excess sugar from liver • Average age 30-50 • Typically heavy • Genetically set up ”survivor” • 90% of people with diabetes @ Dx: 50% less insulin produced High BP High Trigs/ High LDL/ Low HDL
Insulin resistance Insulin deficiency Excessive hepatic glucose release Understanding Diabetes:Type 2
Type 2 Diabetes Insulin resistance How will you know? “undertall” Insulin deficiency How will you know? BS fasting, before and after eating Excessive hepatic glucose release How will you know? BS fasting
Type 2 Diabetes Insulin resistance Insulin Sensitizers Insulin deficiency Incretins: Victoza Byetta Januvia Onglyza Tradjenta Meglinitides Sulfonylureas AGI’s Excessive hepatic glucose release Metformin
Ooodals of meds- where do we start? ADA Says: • At diagnosis: • Lifestyle therapy (1-800-DIABETES ED) and Metformin • If A1c not under 7%: • Add either sulfonylurea or insulin • But not glyburide or chlorpropamide • Then intensify insulin therapy • Continue metformin- IT HELPS!!!! ITS CHEAP!!! WEIGHTLOSS!! • Drop SU once using intensified insulin regimen
ADA Treatment Algorithm • “Less Well-Validated therapies”(i.e. last ditch effort before insulin) • We can’t prove longterm benefit with these meds • TZDs (Actos, Avandia) • Incretins • No hypoglycemia • No weight gain, but no weight loss • Similar potency to SU; not more • Expensive
GLP-1 Incretin System Increase insulin secretion Suppresses glucagon secretion FBS & PP blood sugars hunger, slows gastric emptying Small Intestine Incretins
“Bad diabetes” is the kind where you take insulin Hog Wash... • Insulin is not the enemy, HIGH BLOOD SUGAR is! • Over time, many people with diabetes need insulin because the pancreas “poops out.” • Can’t “squirt it out?” Gotta “squirt it in.” • “Good diabetes” is CONTROLLED diabetes, regardless of the treatment.
Insulin is not the bad guy • Insulin: “Use Early and Often” • Physiologic timing pattern of normal insulin • Basal-bolus regimens: • Education required • Allows flexibility • Consider Co-management with Endocrinology and with Diabetes Education Program
The “5 Rights” of Insulin Therapy • The Right insulin • Rapid acting, long acting? • At the Right time • Where is insulin needed? Food? Background? • In the Right amount • Carb coverage/ Premeal adjustment/Background • With the Right device • Short Needles, Small syringes, Pens, Pumps • For the Right to live life well with diabetes
AcanthosisNigricans (AN) Cause- High insulin levels in bloodstream Cure- Decrease Insulin Levels in Blood
Feelings and Diabetes • Some common myths: • Diabetes destroyed my plans and dreams. • Asking for help is a sign of weakness. • I should be able to take diabetes in stride. • I should hide my diabetes from others. • The truth: • People with diabetes have depression almost twice as often as people without. • People want to help- ask!!
Spotting Depression • Increase in readmissions • Not sleeping/sleeping too much • Appetite changes • 4. Guilt statements, hopeless statements • 5. Suicidal thoughts/statements • Drug/alcohol use • 7. Less family/friends visiting when they are in the hospital • 8. Not performing ADLs, not picking up meds at pharmacy, missing appointments • 9. No mention of friends, family, hobbies • 10. Recent bad news- lost a job, lost a loved one, lost more of their health • 11. Use a depression tool/or ASK THEM. • "This is a hard disease. It takes a lot of work. You have had it a long time. Does it get you down?"
Eating Disorders & Diabetes Diabulemia- a condition when insulin dosing is inadequate for the purpose of losing weight -Food Hoarding -Lack of Pleasure in eating food
Thank You! • Any Questions?????