Download
1 / 1
10 likes | 108 Views
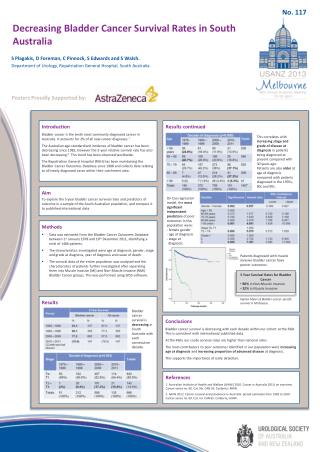
No. 076. A 10-year Histopathological Audit of Radical Cystectomy in a Single Pathology Centre in New South Wales, Australia. Nariman Ahmadi , Warick J Delprado , Andrew J Brooks, Phillip C Brenner, Alexander Grant, Graham M Coombes, Manish I. Patel

E N D
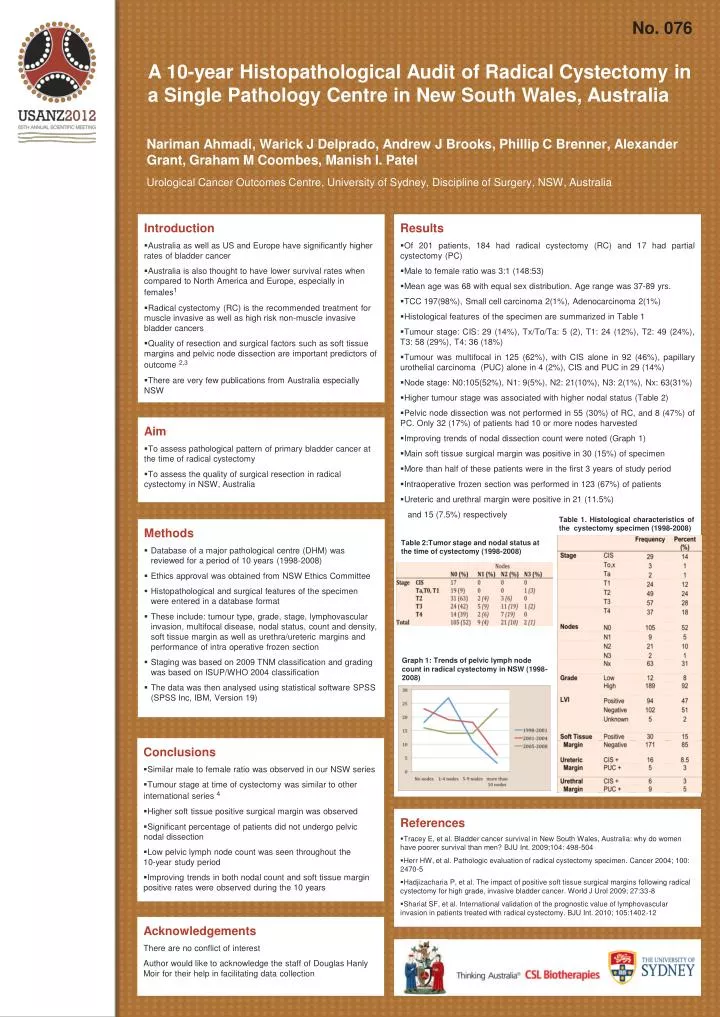
No. 076 A 10-year Histopathological Audit of Radical Cystectomy in a Single Pathology Centre in New South Wales, Australia NarimanAhmadi, Warick J Delprado, Andrew J Brooks, Phillip C Brenner, Alexander Grant, Graham M Coombes, Manish I. Patel Urological Cancer Outcomes Centre, University of Sydney, Discipline of Surgery, NSW, Australia • Introduction • Australia as well as US and Europe have significantly higher rates of bladder cancer • Australia is also thought to have lower survival rates when compared to North America and Europe, especially in females1 • Radical cystectomy (RC) is the recommended treatment for muscle invasive as well as high risk non-muscle invasive bladder cancers • Quality of resection and surgical factors such as soft tissue margins and pelvic node dissection are important predictors of outcome 2,3 • There are very few publications from Australia especially NSW • Results • Of 201 patients, 184 had radical cystectomy (RC) and 17 had partial cystectomy (PC) • Male to female ratio was 3:1 (148:53) • Mean age was 68 with equal sex distribution. Age range was 37-89 yrs. • TCC 197(98%), Small cell carcinoma 2(1%), Adenocarcinoma 2(1%) • Histological features of the specimen are summarized in Table 1 • Tumour stage: CIS: 29 (14%), Tx/To/Ta: 5 (2), T1: 24 (12%), T2: 49 (24%), T3: 58 (29%), T4: 36 (18%) • Tumour was multifocal in 125 (62%), with CIS alone in 92 (46%), papillary urothelial carcinoma (PUC) alone in 4 (2%), CIS and PUC in 29 (14%) • Node stage: N0:105(52%), N1: 9(5%), N2: 21(10%), N3: 2(1%), Nx: 63(31%) • Higher tumour stage was associated with higher nodal status (Table 2) • Pelvic node dissection was not performed in 55 (30%) of RC, and 8 (47%) of PC. Only 32 (17%) of patients had 10 or more nodes harvested • Improving trends of nodal dissection count were noted (Graph 1) • Main soft tissue surgical margin was positive in 30 (15%) of specimen • More than half of these patients were in the first 3 years of study period • Intraoperative frozen section was performed in 123 (67%) of patients • Ureteric and urethral margin were positive in 21 (11.5%) • and 15 (7.5%) respectively • Aim • To assess pathological pattern of primary bladder cancer at the time of radical cystectomy • To assess the quality of surgical resection in radical cystectomy in NSW, Australia Table 1. Histological characteristics of the cystectomy specimen (1998-2008) • Methods • Database of a major pathological centre (DHM) was reviewed for a period of 10 years (1998-2008) • Ethics approval was obtained from NSW Ethics Committee • Histopathological and surgical features of the specimen were entered in a database format • These include: tumour type, grade, stage, lymphovascular invasion, multifocal disease, nodal status, count and density, soft tissue margin as well as urethra/ureteric margins and performance of intra operative frozen section • Staging was based on 2009 TNM classification and grading was based on ISUP/WHO 2004 classification • The data was then analysed using statistical software SPSS (SPSS Inc, IBM, Version 19) Table 2:Tumor stage and nodal status at the time of cystectomy (1998-2008) Graph 1: Trends of pelvic lymph node count in radical cystectomy in NSW (1998-2008) • Conclusions • Similar male to female ratio was observed in our NSW series • Tumour stage at time of cystectomy was similar to other international series 4 • Higher soft tissue positive surgical margin was observed • Significant percentage of patients did not undergo pelvic nodal dissection • Low pelvic lymph node count was seen throughout the 10-year study period • Improving trends in both nodal count and soft tissue margin positive rates were observed during the 10 years • References • Tracey E, et al. Bladder cancer survival in New South Wales, Australia: why do women have poorer survival than men? BJU Int. 2009;104: 498-504 • Herr HW, et al. Pathologic evaluation of radical cystectomy specimen. Cancer 2004; 100: 2470-5 • Hadjizacharia P, et al. The impact of positive soft tissue surgical margins following radical cystectomy for high grade, invasive bladder cancer. World J Urol 2009; 27:33-8 • Shariat SF, et al. International validation of the prognostic value of lymphovascular invasion in patients treated with radical cystectomy. BJU Int. 2010; 105:1402-12 Acknowledgements There are no conflict of interest Author would like to acknowledge the staff of Douglas Hanly Moir for their help in facilitating data collection