Download
1 / 23
320 likes | 594 Views
STATUS OF DETECTION OF MINIMAL RESIDUAL DISEASE (MRD) IN ACUTE LYMPHOBLASTIC LEUKEMIAS. DEPT OF MOL ONCOLOGY. CANCER INSTITUTE (WIA) ADYAR, CHENNAI - 600 020. INTRODUCTION. ALL MOST COMMON PEDIATRIC MALIGNANCY REGISTERED AT CANCER INSTITUTE (WIA)

E N D
STATUS OF DETECTION OF MINIMAL RESIDUAL DISEASE (MRD) IN ACUTE LYMPHOBLASTIC LEUKEMIAS DEPT OF MOL ONCOLOGY CANCER INSTITUTE (WIA) ADYAR, CHENNAI - 600 020
INTRODUCTION • ALL MOST COMMON PEDIATRIC MALIGNANCY REGISTERED AT CANCER INSTITUTE (WIA) • 30-40% T-ALL- WESTERN STUDIES – 85% B-ALL AND 15% T-ALL • MCP 841 –80-90 % ACHIEVE CR BUT 30-40% RELAPSE • PERSISTENCE OF LOW NUMBERS OF RESIDUAL LEUKEMIC CELLS – NOT DETECTABLE BY CONVENTIONAL CYTOMORPHOLOGICAL METHODS (1-5%) • NEED FOR A SPECIFIC AND SENSITIVE METHOD TO DETECT/DEFINE MOLECULAR REMISSION/ RELAPSE (MINIMAL RESIDUAL DISEASE)
DETECTION OF MINIMAL RESIDUAL DISEASE IN T-ALL • WHY DETECT MRD? • HELP ANTEDATE RELAPSE. • THERAPY STRATIFICATION • RISK STRATIFY PATIENTS • ASSESS RESPONSE TO TREATMENT • INTRODUCTION OF NEWER FORMS OF • BIOLOGICAL THERAPY WHEN TUMOUR • LOAD IS LOW • EVALUATION AS A PROGNOSTIC MARKER
MARKERS USED FOR MRDIN ALL • PCR ANALYSIS OF CLONE SPECIFIC • JUNCTIONAL REGIONS OF TCR AND GENE • REARRANGEMENTS • PCR ANALYSIS OF BREAKPOINT FUSION • TRANSCRIPTS OF LEUKEMIA SPECIFIC • CHROMOSOMAL ABERRATIONS (BCR-ABL, • TEL-AML,E2A-PBX, MLL-AF4. TAL-1 DELETION) • MULTI PARAMETER FLOW CYTOMETRY • QUALITATIVE AND QUANTITATIVE
TCRgANDd GENE REARRANGEMNTS DIVERSITY OF TCR BY T CELL DIFFERENTIATION-CORTICAL THYMOCYTES--V-D-J RECOMBINATION Germline J1 V V D J 1 V 1-J1 V1-J 1 Rearranged JUNCTIONAL REGION JUNCTIONAL REGION T-ALL ARREST IN DIFFERENTIATION CLONAL PROLIFERATION OF ARRESTED CELL EACH CELL IN CLONE --IDENTICAL JUNCTIONAL SEQUENCE
TCRgANDd ARE GOOD MARKERS FOR MRD – PCR • LIMITED GERMLINE AND COMBINATORIAL DIVERSITY • OF TCR AND GENES BUT EXTENSIVE JUNCTIONAL • REGION DIVERSITY (LEUKEMIA SPECIFIC DNA • FINGERPRINT) - DIFFERENT IN EACH LYMPHOCYTE • AND EACH LYMPHOID LEUKEMIA. • DEVISE PATIENT SPECIFIC PRIMERS/PROBES(ASO) • SOMATIC MUTATIONS NOT REPORTED IN • REARRANGED TCR GENES • IN 95% OF T-ALL, REARRANGED TCR AND • JUNCTIONAL REGIONS OR BOTH ARE USED AS • TARGETS FOR MRD-PCR
PITFALLS IN THE USE OF JUNCTIONAL REGIONS AS MRD PCR TARGETS • FALSE POSITIVE • BACKGROUND AMPLIFICATION OF SIMILAR • REARRANGEMENTS IN POLYCLONAL REACTIVE T • LYMPHOCYTES / NORMAL LYMPHOCYTES • HETERO DUPLEX ANALYSIS – SIMPLE, FAST • CHEAP, RELIABLE METHOD TO CONFIRM • CLONALITY
DETECTION OF MINIMAL RESIDUAL DISEASE • INSTITUTE EXPERIENCE • GENOMIC DNA -NORMAL & LEUKEMIC CELLS • QUANTITATION -DIAGNOSIS , REMISSION, NORMAL • ( SPEC) • PCR AMPLIFICATION OF ABL, TCR AND TCR AT • PRESENTATION • HETERODUPLEX ANALYSIS—PAGE • HD BAND CUT ,ELUTED ,PCR REAMPLIFIED AND • SEQUENCED TO DESIGN ASO (ALLELE SPECIFIC OLIGO)
DETECTION OF MINIMAL RESIDUAL DISEASE IN T-ALL -PCR-HDA • 50 CASES OF T-ALL STUDIED AT PRESENTATION • PCR–CLONALITY CONFIRMED BY HD ANALYSIS • 24 CASES WERE AVAILABLE FORFOLLOW-UP STUDIES • DURATION OF FOLLOW-UP FROM 6 TO 72 MONTHS • V1-J11.3/2.3 62.5% • V1 - J1 64% • 2 V CLONAL MARKERS 17.5% • V-J1 AND V1-J11.3/2.3 46%
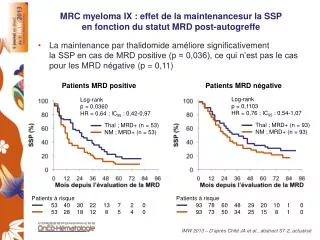
MRD-PCR FOLLOW UP – REMISSION / RELAPSE • ALL PATIENTS WERE PCR +VE/HD +VE AT END • OF INDUCTION THERAPY (3 MOS) -MCP 841 • 6 PATIENTS IN CR BUT REVEALED CONTINUOUS • PCR +VE/ HD +VE RELAPSED AND DIED • COMBINATION OF PCR PRODUCTS AT • PRESENTATION AND RELAPSE - SAME HD • PATTERN - IDENTICAL CLONALITY • ALL PATIENTS IN LONG TERM CR WERE HD –VE • IN 8-12 MONTH REMISSION SAMPLES AND • CONTINUED TO BE PCR –VE/HD -VE Leukemia Research 2002 Vol 26, 335-43
RESULTS - MRD IN T-ALL-MCP 841 LEUKEMIA rESEARCH
HETERODUPLEX ANALYSIS hetero homo homo
QUANTITATION OF MRD • DETECT AND ACCURATELY ASSESS THE • VOLUME OF PERSISTENT SUB -CLINICAL • DISEASE -LEVELS AND DYNAMICS OF MRD • DEFINE THE EXTENT OF REDUCTION IN • TUMOR VOLUME REQUIRED TO PREVENT • RELAPSE AND ENSURE LONG TERM DISEASE • FREE SURVIVAL • COMPETITIVE PCR • LIMITING DILUTION • REALTIME PCR LABORIOUS, MORE AMOUNT OF DNA , RISK OF CONTAMINATION
QUANTITATION OF MRD – REAL TIME Q-PCR • AFFORDS BOTH AMPLIFICATION AND ACCURATE QUANTIFICATION DURING EXPONENTIAL PHASE OF INITIAL TARGETS - SHORT TIME • FLOURESCENCE IS MONITORED AND THE CROSSING POINT/THRESHOLD CORRELATES TO AMOUNT OF INITIAL COPIES OF TARGET • NO NEED FOR GELS, RADIOACTIVITY AND POST -PCR MANIPULATION • DETERMINATION OF LARGE DYNAMIC RANGE OF STARTING TARGET MOLECULE DETERMINATION
REAL TIME PCR TECHNIQUES • SYBER GREEN 1 -BINDS TO DOUBLE STRANDED DNA • HYBRIDISATION PROBE – DONOR AND ACCEPTOR FLUROCHROMES-FRET • HYDROLYSIS PROBE -TAQMAN PROBE- 5’-3’ NUCLEASE ACTIVITY OF TAQ POLYMERASE Q R 3 5 Fl emitted Fl quenched
REAL TIME PCR -QUANTITATION OF MRD 1 ASO- PCR - SPECIFICITY AND SENSITIVITY ( 1 IN 10-5 ) 2 ASO-PCR NORMAL DNA-NON SPECIFIC AMPLIFICATION 3 STANDARD CURVE PCR WITH KNOWN INTERNAL CONTROL-(RNASE P)(50 ng--50 pg) QUANTITATE SAMPLES 4 STANDARD CURVE PCR WITH ASO-J1 –SERIAL DILUTION OF PRESENTATION LEUKEMIC DNA (50ng--5pg) IN 500ng OF NORMAL DNA. 5 REMISSION SAMPLE QUANTITATED USING ABOVE STD CURVE
WHEN AND HOW OFTEN SHOULD MRD BE MONITORED • SINGLE TIME POINT ANALYSIS IS INADEQUATE • AT LEAST 2 SERIAL MEASUREMENTS ARE NEEDED DURING EARLY MONTHS OF TREATMENT • AT END OF INDUCTION 1-RESPONSE TO TREATMENT • AT START OF CONSOLIDATION-RISK OF RELAPSE IS PROPORTIONAL TO MRD LEVELS-POWERFUL PROG NOSTIC MARKER • LOW RISK 10-3 INTERMEDIATE RISK 10-3 HIGH RISK 10-2 • SLOWER KINETICS OF CLEARANCE IN T-ALL COMPARED TO PRE-B -ALL PROGNOSTIC VALUE OF MRD IN ALL
FUTURE STUDIES MICROARRAYS
THIS STUDY WAS FUNDED BY THE NCI GRANT FRA No N427-645 AND THE DEPARTMENT OF SCIENCE AND TECHNOLOGY, GOVT OF INDIA THANKS TO Dr T RAJKUMAR, SCIENTIFIC DIRECTOR MR SUDHAKAR, SRF IN THE DEPT DR RAJALEKSHMY, HEMATOPATHOLOGIST MISS MEENA , GRADUATE TECHNICIAN DR T G SAGAR ,DR ANITHA & DR S G RAMANAN DR V SHANTA, CHAIRMAN , CANCER INSTITUTE(WIA)