Download
1 / 19
190 likes | 296 Views
Medical Necessity and One Day Stays Initiative. Alan L. Wang, MD Chief Medical Officer, EJCH Co-Director, Hospital Medicine, EJCH Elaine Cooke, RN Director, Case Management / Utilization Management, EJCH. History of the Initiative.

E N D
Medical Necessity and One Day Stays Initiative Alan L. Wang, MD Chief Medical Officer, EJCH Co-Director, Hospital Medicine, EJCH Elaine Cooke, RN Director, Case Management / Utilization Management, EJCH
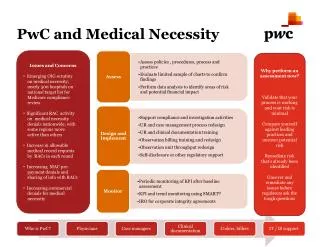
History of the Initiative • CMS began an intensive process improvement plan to reduce payment errors from Medicare One Day stays. • QIOs are conducting projects related to medical necessity of inpatient admissions for CMS. • Several of the HCA hospitals are now under QIO review and more will be added in the future. • Incorrect admission status may incur further monetary penalties to patients.
What is observation? • Use of a bed and periodic monitoring by hospital staff to evaluate an outpatient’s condition to determine the need for possible inpatient admission.
Does observation require a doctor’s order? • Yes. • Dated and timed. • Order should be written PRIOR to the initiation of observation services.
How should the order be written for obs vs. inpatient? • “Place in observation.” • “Admit as inpatient.”
When is observation appropriate? • Physician needs additional time to evaluate to determine need for inpatient. • Physician feels patient may respond rapidly to treatment. • Complication from outpatient surgery.
What services would qualify for observation? • Medical Necessity • Documented in the chart
What does NOT qualify for observation? • Routine stays after late surgery • Diagnostic testing • Outpatient therapy/procedures • Convenience of patient/family/doctor • Admitting to observation prior to outpatient procedure • Staying past the 48th hour • Awaiting placement
How many hours will Medicare cover for Observation? • May NOT exceed 48 hours • Decision to release or admit should e made within 24 hours. • Rarely, 48 hours
Ca you change from inpatient to obsevation? • Medicare • Change/Order made/clarified PRIOR to discharge • Physician’s concurrence documented in chart.
What post-op complications may warrant observation? • Persistent N/V • Fluid/electrolyte imbalance • Uncontrolled pain • Arrhythmias • Excessive/uncontrolled bleeding • Psychotic behavior • Unstable LOC • Deficit in mobility/coordination
Can an outpatient surgery patient be admitted to observation? • No complications • NO…not used as a substitution for the recovery room.
Does the hospital get reimbursed for observation? • Yes. • Medicare for example • “packaging” of services
Why did Medicare package observation services? • CMS noted abuse of observation • Used inappropriately • Remaining in observation for days • Leads to payment errors
Observation Examples • Adominal pain not surgical • Allergic reaction, generalized • AMS • Anemia • Asthma • Atypical CP • Back Pain • Complications post outpatient surgery • Epistaxis • HA
More Observation Examples • HTN • Renal colic • Near drowning (no AMS) • Smoke inhalation • N/V (dehydration) • R/O any condition • TIA • Weakness/dizziness/syncope • Urinary retention requiring cath • Vaginal bleeding
Prevention of Errors • Multidisciplinary rounds on M, W, F at 11:30 am • Meetings with case management representative T, R, Sa and Su • Case management, Case management, Case management!
Summary (What can I do to help?) • Date and time admit order • Specify level of care…”place in observation” or “admit as inpatient” • Make decision within 24 hours to either admit or discharge • For outpatient surgery with complications, document need for furthering monitoring for observation. • Physician and hospital should bill the same status.