Download
1 / 15
150 likes | 571 Views
A Comparison Between Two Leading Stereotactic Platforms in the Treatment of Multiple Metastases. Sandra Vermeulen MD, James Raisis MD, Francisco Li MS, Per Kj ä ll PhD Northwest Hospital Gamma Knife, Seattle Seattle Cyberknife, Seattle R & D Physics, Eletka Instruments AB, Stockholm, Sweden.

E N D
A Comparison Between Two Leading Stereotactic Platforms in the Treatment of Multiple Metastases Sandra Vermeulen MD, James Raisis MD, Francisco Li MS, Per Kjäll PhD Northwest Hospital Gamma Knife, Seattle Seattle Cyberknife, Seattle R & D Physics, Eletka Instruments AB, Stockholm, Sweden
Precision Reproducibility Operator Friendly Patient comfort Treatment time constraints Frame, No frame Radiosurgical Stereotactic Platform Objectives
Approved by the FDA since 2001 More than 120 hospitals and medical centers provide CyberKnife technology Greater than 40,000 patients treated worldwide More than 400 peer review papers have been published Patient mix: 50% cranial, 50% extra-cranial Cyberknife Credentials
No immbolization frame Real-time imaging required Motion tracking required Capable of Fractionation important if tumors engulf optic apparatus, spinal cord or other sensitive structures Large tumors Extra-cranial targeting below the clavicle possible More staffing requirements More complex QA requirements Cyberknife Characteristic that Differ from Gamma Knife
Most patients have multiple lesions MRI screening evaluations show 80% of patients have more than 1 metastases and 50% have 3 or more Many patients require more than one SRS session during the course of their disease Are CK and GK beam profiles the same for 1, 4 or 10 metastases? Brain Metastases
Defined in the RTOG radiosurgical guidelines 90-05 as a measure of the conformity of the Prescribed Dose (PIV) to the Target Volume (TV). Index Conformity (PIV/TV ratio) of Radiosurgical Treatment Plans
CK cone diameters (mm) available: 5, 7.5, 10, 12.5, 15, 20, 25, 30, 35, 40, 50, 60 An output factor is a ratio of dose for a given field size to that for a reference field size The output factor of the 5 mm cone has not been verified by the manufacturer CK Cone Size Selection
MH is a 35y/o mother of 2 with a 4 year history of metastatic breast cancer involving brain, lung and bone. Systemic treatment includes chemotherapy, monoclonal antibodies and hormones SRS by CK has been given twice for BM (6 lesions have been treated over 2 years) Patient has been followed for 6 months with 10 intracranial lesions, all under 1 cm With a continued KPS of 80%, patient has refused WBRT because of the risk of dementia and the GK because of the frame placement Extreme Brain Metastases Case
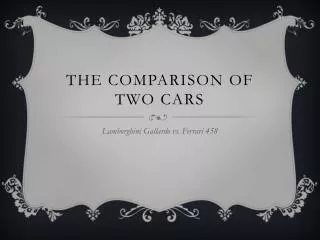
CyberKnife: Single Matrix and Multiple Matrix Plans Single Matrix Multiple Matrix
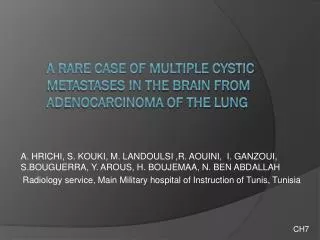
Cyberknife: Conformity Index Multiple and Single Matrix Multiple Matrix, 2.08 CI/2.17 nCI Single Matrix, 1.68 CI/1.70 nCI
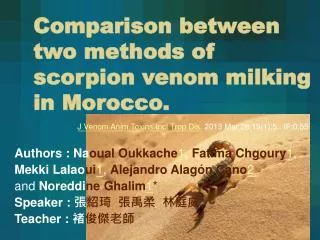
Gamma Knife: Single Matrix and Multiple Matrix Plans Multiple Matrix, nCI 1.04 Single Matrix, nCI 1.14
When treating more than 4 lesions, target conformity is lost and normal brain inclusion within lower non-prescription isodose volumes is increased. Output measurement of 5 mm cone not verified by manufacturer (most center do not treat tumors smaller than 4 mm’s) Cyberknife Limitations in the Treatment of Multiple Metastases
The dosimetry of either GK or CK in the treatment of < 4 metastases which are greater than 5 mm’s is comparable by radiosurgical standards When treating > 4 metastases, a larger number of lesions can be treated with GK than CK with better dosimetry and less normal brain inclusion within lower isodose volumes. Conclusion