Download
1 / 23
230 likes | 453 Views
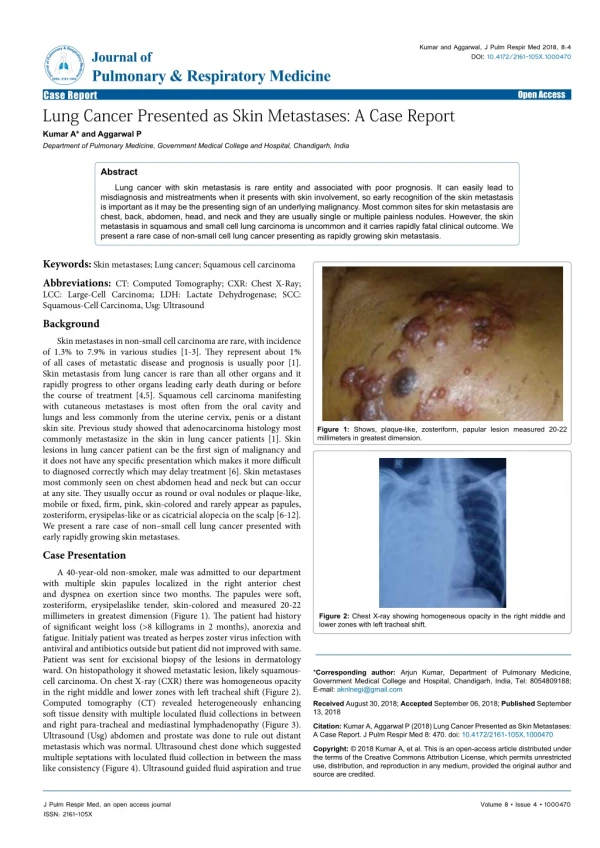
A. HRICHI, S. KOUKI, M. LANDOULSI ,R. AOUINI, I. GANZOUI, S.BOUGUERRA, Y. AROUS, H. BOUJEMAA, N. BEN ABDALLAH Radiology service, Main Military hospital of Instruction of Tunis, Tunisia. A RARE CASE OF MULTIPLE CYSTIC METASTASES IN THE BRAIN FROM ADENOCARCINOMA OF THE LUNG . CH7. Inroduction :.

E N D
A. HRICHI, S. KOUKI, M. LANDOULSI ,R. AOUINI, I. GANZOUI, S.BOUGUERRA, Y. AROUS, H. BOUJEMAA, N. BEN ABDALLAH Radiology service, Main Military hospital of Instruction of Tunis, Tunisia A RARE CASE OF MULTIPLE CYSTIC METASTASES IN THE BRAIN FROM ADENOCARCINOMA OF THE LUNG CH7
Inroduction: Severaldiseasescan present with multi-cystic brain lesions: • True cysts • Abscess formations • Cysticercosis • Fungal infections • Cerebral tumors • Metastases…
Radiologistrole? 1- Positive diagnosis easy! 2- Approach of etiologicdiagnosis: the main question!
Case report: A rare case of cystic intracerebral metastases from adenocarcinoma of the lung
♂ • 49 yearsold • No medical histories • Smoking patient • Presented with progressive dizziness and equilibrium disorders that had developed for 5 days.
Neurological examination: • cerebellar syndrome • no other focal signs Biology: • Lymphocytes: ↓ • Alkaline phosphatase: ↑ • Other laboratory studies: normal CT brain Scan was indicated
CT brain scan without(a) and with(b) injection of iodinated contrast: multifocal hypodense lesions(a) with partial peripheral contrast enhancement(b) but without significant perifocaloedema. Imaging findings: a1 b1 a2 b2
Further brain MRI was performed and allowed to objectify: multifocal cystic lesions with partial peripheral contrast enhancement but without significant perifocaloedema.
a1 a2 a3 b1 b2 b3 Axial T1-weighted with (a1, a2, a3) and without gadolinium (b1, b2, b3):nodularhypointense multiple extra-axial lesions, with partial peripheral contrast enhancement.
a1 a2 a3 b1 b2 b3 Axial T2-weighted (a1, a2, a3) and FLAIR (b1, b2, b3): Multiple hyper-T2 hypo-FLAIR extra-axial lesions (cysticlesions).
a1 a2 a3 b1 b2 b3 axial diffusion (a1, a2, a3) and ADC (b1, b2, b3): Multiples nodularlesionshyperintense in diffusion with a low ADC.
In total: • ♂ • 49 yearsold • No medical histories • Smoking patient • Lc ↓ , PAL ↑ • multi-cystic brain lesions (CT – MRI) ????
In total: • ♂ • 49 yearsold • No medical histories • Smoking patient • Lc ↓ , PAL ↑ • multi-cystic brain lesions (CT – MRI) ???
In total: • ♂ • 49 yearsold • No medical histories • Smoking patient • Lc ↓ , PAL ↑ • multi-cystic brain lesions (CT – MRI) ??
In total: • ♂ • 49 yearsold • No medical histories • Smoking patient • Lc ↓ , PAL ↑ • multi-cystic brain lesions (CT – MRI) ?
Lung cancer? In total: • ♂ • 49 yearsold • No medical histories • Smoking patient • Lc ↓ , PAL ↑ • multi-cystic brain lesions (CT – MRI)
a CT-chest-scan revealed a lungular small nodule not exceeding 12mm of main line with no other secondary locations • Stereotaxic brain biopsy confirmed a well-differentiated lung adenocarcinoma
Discussion: • Brain lesions in patients with known malignancies are suspicious for metastases; → usually: as well-circumscribed densely enhancing masses with surrounding vasogenic edema. • Cystic brain lesions are unusual; → can be misdiagnosed as: brain abscesses, primary cerebral tumors, or parasitic infections, especially in patients without a history of malignancy.
Cystic cerebral metastases have been described in carcinomas of : • Thymus • Breast • Prostate • Pancreas
However, and in reviewing the literature: -We have only found 2 similar cases reports of lung adenocarcinoma with cystic cerebral metastases. -In both of them, the patients were already followed for bronchial adenocarcinoma. - while in our case, cystic cerebral metastases revealed the disease.
Conclusion: This case demonstrates an unusual pattern of cerebral metastases of a bronchial adenocarcinoma. This constellation should be considered in the differential diagnosis of cerebral cystic lesions even in patients without a history of malignancy, and wich is necessary to evoke at every smoking adult's of about forty. The exact nature of which might be difficult to assess without biopsy.
References: 1-Monabati A, Kumar PV, Kamkarpour A. Intraoperativecystodiagnosis of metastatic brain tumors confused clinically with brain abscess (A report of three cases). ActaCytol. 2000;44:437–441 2-Nieder C, Grosu AL, Grzadziel A, et al. Brain metastases in renal cell cancer: diagnostic and therapeutic aspects. Am J Clin Oncol. 2004;27:632–634 3-White AC, Dakik H, Diaz P. Asymptomatic neurocysticercosis in a patient with AIDS and criptococcal meningitis. Am J Med. 1995;99:101–102 4-Cosgrove SE. Cases from the Osler Medical Service at Johns Hopkins University. Am J Med. 2002;113:158–160 5-Ersahin M, Kilic K, Gögüsgeren MA, et al. Multiple brainmetastasesfrommalignantthymoma. J Clin Neurosci. 2007;14:1116–1120 6-Tsai V, Kim S, Clatterbuck RE, et al. Cystic prostate metastases to the brain parenchyma: report of two cases and review of the literature. J Neurooncol. 2001;51:167–173 7-De Shields MS, Ruether J. Lung carcinoma presenting as multiple cystic lesions in the brain. Del Med J. 1998;70:77–80 8-A.Surov, M Hainz, M Kornhuber . Multiple cystic metastases in the brain from adenocarcinoma of the lung.The American Journal of Medicine. 2009;122:3-4