Download
1 / 29
290 likes | 548 Views
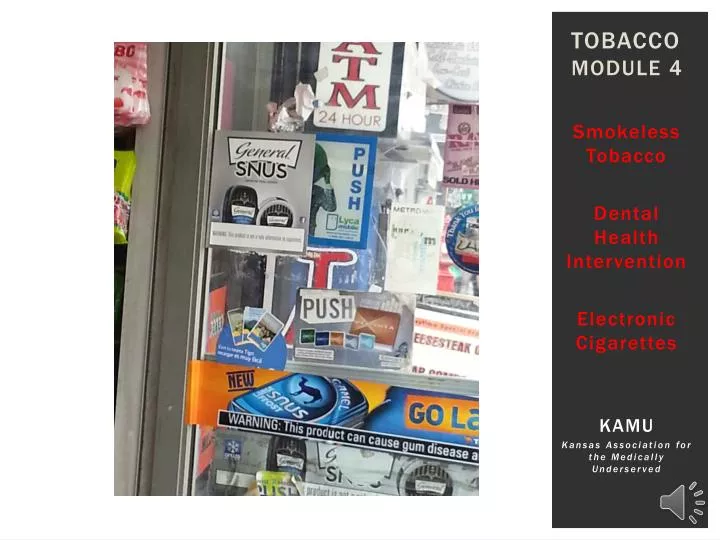
Tobacco Module 4. Smokeless Tobacco Dental Health Intervention Electronic Cigarettes KAMU Kansas Association for the Medically Underserved. Goals: Tobacco Cessation Training Community Health Clinics. Module 1: Why is it Hard to Q uit ? Module 2: Ask, Advise, Assist, Refer

E N D
TobaccoModule 4 Smokeless Tobacco Dental Health Intervention Electronic Cigarettes KAMU Kansas Association for the Medically Underserved
Goals: Tobacco Cessation TrainingCommunity Health Clinics • Module 1: Why is it Hard to Quit? • Module 2: Ask, Advise, Assist, Refer • Module 3: Quit Smoking Medications • Module 4: Smokeless Tobacco, Dental Health Intervention and E-cigarettes • Module 5: Office Systems and Creating a Quit Plan Babalola Faseru, MD, MPH Department of Preventive Medicine and Public Health University of Kansas Medical Center
Objectives • Types of Smokeless Tobacco • Prevalence, Health Effects, and How to Treat • “Ask, Advise, Refer” Model for Dental Practice • E-cigarettes • What we know • What we don’t know • What do you tell your patients
Babalola Faseru, MD, MPH Department of Preventive Medicine and Public Health University of Kansas Medical Center Smokeless TobaccoHarmful & Highly Addictive
Types of smokeless tobacco Snus (snoose)—Scandinavian • moist powder tobacco product (place under upper lip—less need to spit) Snus—American • similar to Scandinavian but no regulation Dipping tobacco • moist snuff (lower lip and gums) causes excess saliva, could require spitting Nasal Snuff • Finely ground dry form of tobacco “snuffed” through the nose Chewing tobacco • long strands placed between cheeks, gum, or teeth (plugs, wads, chew) Dissolvables • strips, sticks, orbs and compressed tobacco lozenges
HEALTH EFFECTS OF Smokeless tobacco Cancer Risk • Smokeless tobacco contains 28 carcinogens • Increases the risk of developing several cancers Oral Health Dangers • Increases the risk of developing precancerous mouth lesions • Strongly associated with recession of the gums. Heart Disease and Stroke • Strongly associated with heart disease and stroke Addiction • Use leads to nicotine addiction and dependence http://www.ctri.wisc.edu/HC.Providers/spit/Spit_tobacco_treatment.pdf Leukoplakia
NICOTINE & Smokeless“Holding an average-size dip in your mouth for 30 minutes gives you as much nicotine as smoking three cigarettes. A 2-can-a-week snuff dipper gets as much nicotine as a 1-1/2 pack-a-day smoker does.”http://www.nidcr.nih.gov/OralHealth/Topics/SmokelessTobacco/SmokelessTobaccoAGuideforQuitting.htm Two main types of smokeless tobacco in the U.S. Chewing Tobacco Snuff Snus by Andreas Hagerman
Smokeless tobacco USE in Kansas2010-2011 Gender differences Ethnic differences (high school) African Americans 10.5% Caucasian 9.3% Other race 7.0% Adult: • Males: • Dual use: 13.3% • Exclusively: 5.3% • Females: <1% High school students: Male: 15.5%; Females: <2% Middle school students: Males: 4.1%; Females: <2% Kansas Tobacco Youth Survey, 2010; http://www.kdheks.gov/tobacco/download/YTS2010_FactSheet.pdf Kansas BRFSS Tobacco and Adult Report, 2011; http://www.kdheks.gov/brfss/PDF/2011_BRFSS_Kansas_Tobacco.pdf
Tobacco Company Marketing to youth Chewing Tobacco Candy by Zombieite http://goo.gl/Gp9glg
ST treatment Strategy is different Tobacco Dependence Smokeless Dependence Normal dip or chew contains 3.6 to 4.5 mg nicotine Nicotine in dip or chew takes 30 minutes for the nicotine to be absorbed into system With ST, nicotine continues to be absorbed 60 minutes after the tobacco is removed • Cigarette contains 1.8 mg nicotine • Nicotine from cigarette drag takes 7 seconds to reach brain and dopamine release • Once cigarette is extinguished, individual is no longer receiving nicotine
Evidence-based treatment for adultsCombination of behavioral treatment and NRT is most effective Encourage counseling Identify triggers Modify behaviors that increase risk for relapse
Evidenced-based Treatment for Adults Nicotine Replacement Therapy (NRT) The dose is based on amount of Smokeless Tobacco used/week: The Nicotine Patch • If > 3 cans or pouches of tobacco per week: • Then prescribe a 42 mg patch dose (two 21 mg patches) daily for 4-8 weeks* • If 2-3 cans or pouches of tobacco per week: • Then prescribe the 21 mg patches daily for 4-8 weeks* • If < 2 cans or pouches of tobacco per week: • Then prescribe the 14 mg patches daily for 4-8 weeks* *If patient reports no withdrawal/craving, then taper doses in 7-14 mg steps every 2-4 weeks. EbbertJO, et al. Effect of high-dose nicotine patch therapy on tobacco withdrawal symptoms among smokeless tobacco users. Nicotine Tob Res. 2007;9:43–52. Nicotine Patch for Smokeless Tobacco Users, J. Ebbert et al. Nicotine and Tobacco Research; July 2013
Nicotine Lozenge or Gumto control cravings and withdrawal symptoms Lozenge Gum If the first dip < 30 minutes of awakening, or patient is using >3 cans or pouches of tobacco per week: Prescribe 4 mg Nicotine gum (1-2 pieces) every 1-2 hours as needed If the first dip of the day is > 30 minutes after awakening or patient is using <3 cans or pouches of tobacco per week: Prescribe 2 mg Nicotine gum (1-2 pieces) every 1-2 hours as needed Limit to 10-12 pieces of gum per day. Taper as needed to control cravings and withdrawal symptoms. If the first dip < 30 minutes of awakening, or patient is using >3 cans or pouches of tobacco per week: • Prescribe 4 mg Nicotine lozenge (1-2 pieces) every 1-2 hours as needed If the first dip of the day is > 30 minutes after awakening or patient is using <3 cans or pouches of tobacco per week: • Prescribe 2mg Nicotine lozenge (1-2 pieces) every 1-2 hours as needed Limit use to no more than 20 lozenges/day for up to 12 weeks. Taper as needed to control cravings and withdrawal symptoms. EbbertJO, et al. Effect of high-dose nicotine patch therapy on tobacco withdrawal symptoms among smokeless tobacco users. Nicotine Tob Res. 2007;9:43–52. Nicotine Patch for Smokeless Tobacco Users, J. Ebbert et al. Nicotine and Tobacco Research; July 2013
Combination NRT Therapy Nicotine gum or the nicotine lozenge can be used as needed in combination with the nicotine patch to provide additional control of withdrawal symptoms and cravings. Nicotine gum photo: http://quitgroups.com/2013/10/03/otc-nicotine-replacement-therapies/
Other medications Proven to help quit smoking, jury still out for smokeless: • Bupropion SR: either in combination with NRT products or as monotherapy. • Varenicline: either in combination with NRT products or as monotherapy.
Dental Health Intervention WHY SHOULD DENTAL PRACTICES INTERVENE? Leukoplakia (oral precancer) on floor of mouth and tongue http://www.who.int/oral_health/publications/fact_sheet_tobacco/en/index1.html
Cigarettes and Smokeless harm dental health • Tobacco - major risk factor • oral cancers • periodontal disease, bone and attachment loss • Cigarette smoking slows healing • during periodontal treatment • significantly associated with implant failure
Adam comes to the Dental Clinic • He is 24 • He has never seen a dental hygienist • His workplace is smoke-free • Adam likes to use snus because no one can see it and he doesn't need to spit • Adam’s girlfriend complains of his bad breath • He likes to use a new snus pouch every 3 hours • Note: Adam’s dad used moist snuff for 30 years How can you address Adam’s tobacco addiction?
Dental Health Professional Ask, advise, refer model • ASK: “I see from your health history that you use tobacco.” • “I’d like to show you some changes in your mouth that were caused by your tobacco use.” • ADVISE: “You should stop smoking/using smokeless. Quitting tobacco is one of the most important things you can do to improve your oral health.” • REFER: “I’d like to arrange a visit in our medical clinic to see about medicationsto help you quit. Here is the KANQUIT Quitline number for free, excellent coaching on quitting.” American Dental Hygienists Association; http://www.askadviserefer.org/
Dental and medical clinics Can work together to help tobacco users quit Dental Clinic (AAR) Medical Clinic (AAAR) Ask about tobacco use Advise to quit Referto… Medical clinic provider for medication KS Quitline • Ask about tobacco use • Advise to quit • Assist with medication • Refer to KS Quitline
what’s the buzz? e-cigarettes
Electronic cigarettes • Hand-held devices that mimic the act of smoking • Do not contain tobacco • Battery heats device and makes the tip glow • The user inhales vapor • nicotine, H20, anything else manufacture wants to put in or fails to clean out • “Vaping” Howstuffworks.com
E-Cigarette Use Current users US Adults: “E-cig use began around 2005 and has risen dramatically since that time. By 2011, approximately 2% of all adult Americans used e-cigs, and 1 in 5 American smokers had tried vaping.” High School Students:“According to the CDC’s National Youth Tobacco Survey, the percentage of high school students who reported using an e-cigarette even one time rose from 4.7% in 2011 to 10.0% in 2012.” http://www.ctri.wisc.edu/HC.Providers/healthcare_ecigs.htm http://managedhealthcareexecutive.modernmedicine.com/managed-healthcare-executive/news/cdc-seeks-answers-e-cigarette-use-among-kids#sthash.zuhVJUNW.dpuf
What we know • Known toxins/carcinogens • Some contain tobacco-specific nitrosamines (TSNAs) and diethylene glycol (DEG) • Attractive industry advertising campaigns • “…flavors made in the USA with domestic and imported ingredients.”http://www.blucigs.com/ • Not yet regulated by FDA • Need more testing on long-term health effects • E-liquid or E-juice: Propylene glycol is GRAS, “generally recognized as safe” by the FDA, and used in inhalers, but no one knows the safety of long-term exposure via inhalation
What we Don’t know • Do they have any harms? • How long will it take for evidence-based studies to conclude safety or harm? • Will e-cigs push back gains made on smoke-free environments? • Do e-cigs help smokers quit? • Are smokers “vaping” and continuing to smoke cigarettes? • Would it be fine/desirable for never-smokers to start “vaping”? • What is the impact on our our kids? http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6235a6.htm?s_cid=mm6235a6_w
How to respond to patients questions about e-cigarettesFliPP • Figure out: “What interests you about e-cigarettes?” • Listen and Commend: “It sounds like you’re interested inquitting/cutting down/reducing harm from your tobacco use. That’s great! Stopping smoking is the best thing you can do for your health.” • Inform: 1) Dozens of companies make them 2) Not tested for safety—don’t know what they’re made of or what’s in the vapor 3) Don’t know if they help people stop smoking • Pivot: “For these reasons I can’t recommend e-cigarettes right now, BUT if it’s ok with you, I’ll describe some effective and safe options that are freely available for many patients…” • [e.g., nicotine inhaler, nasal spray, lozenge, gum, patch, other meds] • Plan: “Where would you like to go from here?” • [if patient doesn’t want to try to quit, or wants to try e-cigarettes, ask if you can check in with them later to see how they’re doing] http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm173401.htm
QUIT Plan5a’s Adam and provider can fill out together Support Medications Follow up in 2 weeks Quit date is not necessary
Please take the quiz to complete the module Click on the link below to take you to the quiz for this module Thank you! You may open the survey in your web browser by clicking the link below:Tobacco Module 4 QuizIf the link above does not work, try copying the link below into your web browser:https://redcap.kumc.edu/surveys/?s=Uikjcv Babalola Faseru, MD, MPH Department of Preventive Medicine and Public Health University of Kansas Medical Center