Download
1 / 23
230 likes | 362 Views
CASE 4 “THE DISEASE OF THE SEVENTH DAY”. “THE DISEASE OF THE SEVENTH DAY”.

E N D
“THE DISEASE OF THE SEVENTH DAY” • Baby J.D. is a 7-day old neonate born term in a faraway Bukidnon baragay reachable only by horseback and delivered by a traditional “hilot”. He was admitted because of poor sucking and inability to open the jaw. He was crying excessively and went into spasms when touched. A few hours later, he became highly febrile and his entire body became completely rigid
Questions to be answered • What is the most likely diagnosis of this patient? • Explain the pathophysiology of Tetanus • How is a diagnosis of Tetanus achieved? • What are the differential diagnoses of Tetanus? • What are the goals of treatment of Tetanus? • What are the necessary Preventive measures?
Answer: Neonatal Tetanus • WHO estimates that >500,000 deaths due to Tetanus neonatorum still occurs • Tetanus is an acute toxemic disease caused by Clostridium tetani , a spore forming gram (+) bacillus widely distributed in the soil, animal and human feces, house dust and even in contaminated street drugs.
Neonatal Tetanus • Absence of immunity in the mother and contamination of the umbilical cord account for the occurrence in regions where home delivery is conducted by untrained personnel with the cord cut by an unclean knife, scissors, bamboo etc. and the umbilical stump dressed with earth or animal dung
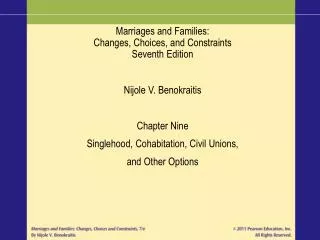
Neonatal Tetanus • Inability to suck, persistent crying, followed by fever and recurrent generalized spasms with deep cyanosis are the usual presenting symptoms Risus sardonicus
Tetanus • The most frequest presenting symptom is painful trismus (lockjaw) due to spasm of the masseter muscles • When the jaw remains tightly clenched together with spasm of the facial muscles, the typical “risus sardonicus” expression results Risus sardonicus
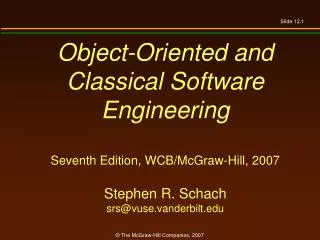
Tetanus • Over the next 24-48 hrs., muscle rigidity spreads to involve the muscles of the neck,back, abdomen and limbs culminating in a very characteristic spasm. • The head is retracted, the spine arches backwards and the abdomen attains a board-like rigidity Opisthotonus • During these spasms, the • child remains mentally alert • but apprehensive • The spasms may be • precipitated by a variety • of stimuli as light or noise
Pathophysiology The potent Tetanus neurotoxin (Tetanospasmin) is synthesized intracellularly. After release it binds to motor end-plates in skeletal muscles. It acts by inhibiting acetylcholine release thereby impairing neuromuscular transmission It reaches the CNS through the perineural spaces of nerve trunks of by hemotagenous dissemination The toxin enters the neurones and becomes irreversibly fixed on to the gangliosides Produces presynaptic inhibition resulting in unopposed muscle contraction and seizures
Diagnosis • The diagnosis of tetanus is entirely clinical • It is often difficult to isolate the bacilli from the wound + the presence of C. tetani does not mean the patient has tetanus (Paediatric Problems in Developing Countries, edited by Robinson M.J)
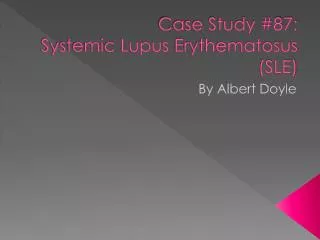
Differential diagnosis of Tetanus • Other convulsive disorders posing a problem in diagnosis: meningitis, phenothiazine dystonia, strychnine poisoning, tetany • Trismus may be seen in rabies Hydrophobia of Rabies
Differential diagnosis of Tetanus Tetany with carpopedal spasm
Q5:What are the goals of treatment in the management of Neonatal Tetanus
Treatment of Neonatal Tetanus Goals of therapy: • Neutralization of toxin still present in the blood before it comes in contact with the CNSantitoxin (human tetanus immune globulin) or Equine antitoxin • Penicillin kills the vegetative forms • Surgical removal of the site of entry of the organism • General measures: mainly supportive • Constant and meticulous nursing care • Control of seizures • Close monitoring of fluid, electrolyte and caloric balance
Treatment of Neonatal Tetanus • Incubator care • External stimulation kept to a minimum but suction of pharyngeal secretions must be done • NGT feeding best avoided during the initial 2-3 days (aspiration precaution) • IVF therapy • Temporary nutritional support with dextrose, amino acids and lipids before onset of gavage feedings • Periodic change of posture • Catheterisation for distended bladder and enemata for constipation
Prevention of Neonatal Tetanus By a combination of: • Improving maternity care with emphasis on increasing the immunization coverage of women of childbearing age esp. pregnant women with tetanus toxoid • Increasing the proportion of deliveries attended by trained attendants
Key Learning Points • Tetanus is a totally preventable disease. Its occurrence is a reflection of the failure of health delivery • Immunization of pregnant mothers at least 6 wks before delivery is the most efficient method of eliminating neonatal tetanus
CASE 4: “The Disease of the Seventh Day”