Download
1 / 111
1.32k likes | 2.08k Views
Carotid Artery Disease . Nathan Orr PGY-4 UK Gen Surgery April 18,2012. Objectives:. Briefly review the history of carotid disease Review treatment recommendations regarding endarterectomy for carotid disease Summarize the literature for endarterectomy (CEA) v. stenting of carotid disease.

E N D
Carotid Artery Disease Nathan Orr PGY-4 UK Gen Surgery April 18,2012
Objectives: • Briefly review the history of carotid disease • Review treatment recommendations regarding endarterectomy for carotid disease • Summarize the literature for endarterectomy (CEA) v. stenting of carotid disease
History of Carotid Disease1875 • Sir William Richard Gowers (British neurologist) • First to link stroke with extracranial vascular disease in 1875 • Described a patient with right hemiplegia and blindness in the left eye • Attributed this syndrome to an occlusion of the left carotid artery in the patient’s neck
History of Carotid Disease1914 • James Ramsay Hunt (American neurologist) emphasized extra cranial carotid artery occlusive disease as a cause of stroke • Urged examination of the cervical portion of the carotid artery during autopsy • Suggested that transient cerebral ischemia was equivalent to intermittent claudication of the brain and represented a prodrome to a major stroke
History of Carotid Disease1934 • EgasMoniz (Portuguese neurologist, Nobel prize 1949) reported that arteriography could be used to diagnose carotid artery occlusion
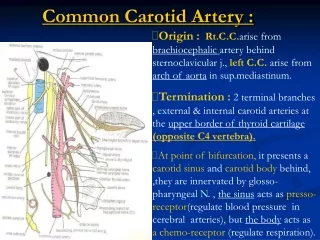
AmaurosisFugax • Temporary monocular blindness (shade coming down over the eye) caused by embolization to the ophthalmic artery • Ulcerated plaque at common carotid bifurcation usual source
Transient Ischemic Attack (TIA) • Defined as any focal neurologic deficit lasting from several seconds to many hours but not longer than 24 hours • Two mechanisms: • Vascular spasm in a partially blocked artery impedes blood flow to the brain temporarily • Small “mini” strokes where pieces of plaque dislodge and embolize • Not benign • Degree of cerebral atrophy and infarction linked to number of TIA’s
TIA and Stroke Risk • 35% of patients with a TIA will have a stroke in their lifetime • 50% of these will occur in the year following first TIA • After first year stroke risk is 5% per year
Stroke • Definition • A sudden loss of brain function caused by an interruption in the supply of blood to the brain. • A ruptured blood vessel or cerebral thrombosis may cause the stroke, which can occur in varying degrees of severity from temporary paralysis and slurred speech to permanent brain damage and death. • Neurologic deficit lasts longer than 24 hours
Stroke • 3rd leading cause of death in the United States • 2nd most common cause of cardiovascular death • #1 cause of death from a neurologic disorder
Stroke • Incidence of new stroke is 160/100,000 • Annual financial impact estimated to be $45.3 billion/year • Death • Disability • Long term care • Medical expenses • Inability to return to previous employment
Stroke • Prognosis • 80% survive initial event • 29% regain normal function • 36% return to work • 18% unable to work, but can take care of themselves • 4% require custodial care • Natural history • only 50% of stroke victims will be alive at five years.
Outcome in patients with asymptomatic neck bruits1986 • NEJM--Chambers BR, et al. • prospectively followed 500 asymptomaticpatients with carotid stenosis ≥ 75% (Doppler) for up to 4 years • 1 year 18% had ischemic cerebrovascular events over ¼ of these events strokes (5.5%) • At 2 years 22% had ischemic cerebrovascular events • In patients with less than 75% stenosis • 1 year 3% with ischemic events • 2 years 6% with ischemic events
Asymptomatic carotid stenosis • What is the risk of stroke with asymptomatic carotid stenosis? • With ≥ 75% asymptomatic stenosis, 22% of patients will have an ischemic cerebrovascular event at 2 years
How can we alleviate the symptoms and results of carotid disease?
Treatment Options… • Medical Management • Carotid Endarterectomy (CEA) • Carotid Artery Stenting (CAS)
Medical Managementfrom the Guidelines for carotid endarterectomy: Circulation 1998;97:501-509 • Both systolic and diastolic blood pressure independently related to stroke incidence • 6mm reduction in DBP produces 42% reduction in stroke rate • Tx of isolated systolic hypertension in patients over 60 reduces stroke incidence by 32% • Smoking cessation • Relative risk 1.5-2.2 • Serum lipid levels • have not been shown to affect stroke rate but low levels slow progression of atherosclerosis
Medical Management • Alcohol consumption • Heavy alcohol use associated with excessive stroke risk • Moderate consumption may have no effect or a slightly protective effect • Antiplatelet therapy • 23% reduction in stroke with aspirin compared to placebo in patients with history of TIA/stroke • Also 22% reduction in MI/death
Carotid Endarterectomy • Surgical removal of the inner layer of the carotid artery when narrowed by atheromatous intimal plaques
History of CEA • KJ Strully attempted (unsuccessfully) to operate on an occluded carotid artery • 1954--First successful extra cranial carotid surgery preformed by Felix Eastcott
History of CEA • In 1953 DeBakey possibly performed the first CEA however it was not published until 1975 • Thus Eastcott is credited with bringing the possibility of carotid artery repair to medical attention.
History of CEA • Dr. Denton Cooley is credited with being the first to use an intravascular shunt during carotid surgery
Questions regarding best treatment • How efficacious is endarterectomy as compared with medical care alone? • Which patients should be offered endarterectomy? • What is the acceptable complication rate? • How durable are the benefits of endarterectomy?
NASCET 1991 • North American Symptomatic Carotid Endarterectomy Trial (50 centers in US and Canada) • Began in 1987, randomized patients to surgical or medical therapy • Stratified patients according to the degree of stenosis • Moderate stenosis (<70%) • Severe stenosis (70-99%)
NASCET 1991 • In 1991 after 659 pts with severe stenosis (>70%) had undergone randomization the stratum was stopped early • Results: • 24% medically managed patients had stroke within 18 months • 7% surgical patients had a stroke within 18 months • Rate of perioperative major stroke/death was 2.1% in this trial
NASCET 1991 • Risk reduction at 2 years with endarterectomy: • 12% for 70-79% stenosis • 18% for 80-89% stenosis • 26% for 90-99% stenosis • Conclusion: • CEA highly beneficial to patients with recent hemispheric and retinal transient ischemic attacks or non disabling strokes and ipsilateral high-grade stenosis (70-99%) of the internal carotid artery
NASCET 1998 • Does CEA benefit symptomatic pts with stenosis <70% • Any ipsilateral stroke at 5 years • 50-69% stenosis • 15.7% CEA • 22.2% medical • <50% stenosis • 14.9% CEA • 18.7% medical (not statistically significant)
NASCET 1998 • Conclusion: • CEA in symptomatic patients with 50-69% yields only moderate reduction in risk of stroke and provided no benefit to patients with <50% stenosis. • Patients with ≥70% stenosis had durable benefit at eight years.
Veterans Affairs Trial, 1993 • Asymptomatic Carotid Stenosis Veterans Administration Study • 11 centers, 1983-1991 • 444 men with asymptomatic carotid stenosis • 50% stenosis or more (angiogram) • Evaluated combined incidence of TIA, AmaurosisFugax, and stroke • Randomized to optimal medical treatment alone vs. optimal medical treatment plus carotid endarterectomy
Veterans Affairs Trial, 1993 Results: Incidence of Neurologic End Points for Ipsilateral Events • All patients followed for an average of 48 months • Incidence of ipsilateral neurologic events • 8% CEA • 20.6% medical group • Stroke/death rate within 30 days not different between groups
ACAS, 1995 • Asymptomatic Carotid Artery Study • Prospective randomized trial • 39 sites in the US and Canada • 1987-1993, 1662 patients with asymptomatic carotid artery stenosis 60% or greater • Daily aspirin administration and medical risk factor management for all patients • Medical vs. carotid endarterectomy
ACAS, 1995 • Outcomes • Cerebral infarction occurring in the distribution of the study artery, any stroke or death • Perioperative risk • 30 days post op 2.3% in the surgery group • Median follow-up 2.7 years • Combined risk of outcomes (stroke, MI, death) • 5.1% CEA • 11% medical management
CEA Summary: • Symptomatic : • Effective for recently symptomatic (within previous 6 months) patients with 70 to 99% ICA angiographic stenosis (Level A) • Should not be considered for symptomatic patients with less than 50% stenosis (Level A) • May be considered for patients with 50 to 69% symptomatic stenosis (Level B) but the clinician should consider additional clinical and angiographic variables • It is recommended that the patient have at least a 5-year life expectancy and that the perioperative stroke/death rate should be <6% for symptomatic patients (Level A) • Medical management is preferred to CE for symptomatic patients with <50% stenosis (Level A)
CEA Summary: • Asymptomatic: • Reasonable to consider CEA for patients between the ages of 40 and 75 years and with asymptomatic stenosis of 60 to 99% if the patient has an expected 5-year life expectancy and if the surgical stroke or death frequency can be reliably documented to be <3% (Level A)
Treatment Options… • Original study designs compared CEA to medical treatment alone • More recently,studies are designed to determine if stenting is equivalent or better than CEA
Carotid Artery Stenting • What is the role of CAS and when is it indicated?
Stent Design • Open Cell • more flexible • conforming • Closed Cell • stiffer • Scaffold and support fractured plaque better • Keep thrombogenic material away from lumen
EPD’s • After 2002, embolic protection devices (EPD’s) were widely used
EPD design • Eccentric filters • Filter placed eccentrically on wire • Better wall apposition leads to better TIA prevention • Concentric filters • Filter placed concentrically on wire
Evaluation of Endovacular Literature: • Types of studies available to review efficacy of stenting • Case series • Industry sponsored registries • Randomized trials
Case Series • Since the advent of CAS in the mid 1990’s • >20 case series of at least 99 patients • Reporting over 24,000 total patients • Weighted avg. showed that 51% of patients treated were symptomatic and >97% received a planned stent • Outcome evaluation by a neurologist was performed in 64%of series
Case Series • 30-day stroke rates varying from 1% to 8% • Overall, average 30-day stroke rate was 3% across all studies • Average combined 30-day rate of stroke, MI, or death was 4% • Early restenosis rates 1%-8% (reported in half the series) • Interpret with caution… • Rates varied with year of procedure, EPD use, neurologist examination, and patient characteristics
Industry-Sponsored Registries • >10 industry-sponsored trials of specific CAS systems have been presented at national meetings • None have been published in a peer-reviewed journal • All (except one) routinely used EPDs • Weighted avg. across the registries showed that 27% of patients were symptomatic
Industry-Sponsored Registries • Stroke rates varied from 2% to 7% at 30 days • Average of 4% of patients experienced peri-procedural strokes • Combined adverse outcomes (stroke, death, or MI) varied from 3% to 8% at 30 days, with a weighted average of 6%