Download
1 / 21
210 likes | 459 Views
Candlelighters Childhood Cancer Foundation. FDA ODAC Subcommittee October 17, 2002. Patient/Family Perspective. Not derived from a formal survey Prospective survey possible Shared perspective Personal experience parent of child with AML (1987)

E N D
Candlelighters Childhood Cancer Foundation FDA ODAC Subcommittee October 17, 2002
Patient/Family Perspective • Not derived from a formal survey • Prospective survey possible • Shared perspective • Personal experience • parent of child with AML (1987) • professional interactions with thousands of families.
Constituency Candlelighters National Office 32 years of serving families – information resource, referrals, and support. • 6,000 phone calls/year • 14,000 email queries/year • 155,000 web site visitors/year • (1.5 million hits).
Specific Inquiries Approximately HALF queries: • Clinical trial information, availability • Institutional referrals • Referral to disease specialists
HopeLink • HopeLink clinical trial search engine on website (www.candlelighters.org) • 385 childhood cancer trials listed, currently open for enrollment. • Comprehensive trial listings; standard and medical formats • eligibility criteria • investigative site locations • contact information
Hope “When the doctor explained to us about Melissa's leukemia, he said that APML is incurable and it’s very rare and very deadly. Can you give us hope?”
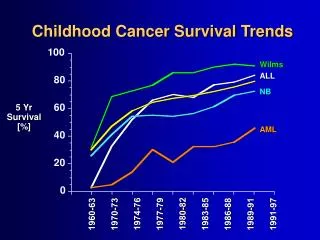
What do families want? • ‘Magic bullet’ to cure child with resistant disease • Options for therapies • Neuroblastoma IV • Brain tumors • Metastatic solid tumors • AML
“ The childhood cancer population is a small community in number, but large in spirit and used to success. The clinical trial process is what has brought pediatric oncology the cures that give hope and help to parents and survivors, and has created a foundation of trust upon which to build improved and novel treatments.” Grace Monaco, Founder CCCF
Timing Access to New Drugs Use of new drugs in recurrent/refractory cases Accurate information built on “foundation of trust”: • Relative safety. • Pre-clinical models, animal testing, adult testing. • Probable tumor response • Possible ‘magic bullet/cure’ vs. actual small percentage response rate to Phase I trials. • Side effects of treatment • Impact on quality of life at probable end of life.
Balance in Decision Making Feedback from families in phase 1 trial experiences (end of life): • Need for greater information • Issue of option of treatment-free death: • Physician should discuss • Ending treatment does not mean “You are a bad parent”. • Ending treatment is not ‘giving up.’ • No ‘heroic’ requirement to ‘go down fighting.’
“To keep the pediatric patient lot improving, the cures growing and the effects of therapy on quality of life, particularly in the hard to handle cancers, we need to innovate within the careful, patient-centered model that pediatricians have always utilized.” Grace Monaco
Barriers to phase 1 pediatric • Industry often un-enthusiastic • Rare pediatric-specific tumor types • Small childhood populations • Problematic access to clinical trial information • Health insurance/billing concerns • Centralized trial information
Innovations: Pediatric Tumors • Perception/action on phase 1 drugs may evolve: • Disparate adult/child tumor types will show similar drug-responsive pathways • Adult CML vs. pediatric medulloblastoma: Gleevec • Emphasis on cross-correlation of genome anatomies (adult, pediatric) • mRNA expression profiles • Genomic DNA somatic mutations • Ensure that pediatric tumors represented in Cancer Genome Anatomy Program (CGAP) and other genomic initiatives.
Adult phase 1 prior to kids? “ There is no reason that the pediatric oncology community should wait for results from any adult trial before designing their own Phase I’s and pilots for the use of new and old agents in pediatric oncology.” Grace Monaco
Adult phase 1 before kids? • In some cases? • Basis for dose initiation • reduce under-dosing/over-dosing of phase I trials • Safety testing
Small Pediatric Population • Formalize coordination of US Adult Cooperative Group Clinical Trial Studies and COG/Academic/Pharmacy Child Studies for Simultaneous Access • Yearly joint symposium on phase 1 trials • Address: Phase 1/in conjunction with palliative care Discussions/documents/consents/assents • Address: Emerging targeted pathways shared by tumors (sub-committees/consortia, data sharing)
Small Pediatric Population… • IF pediatrics is to benefit from greater numbers of adult phase 1 trials • Need much better participation of adults in adult trials • US adult participation in cancer clinical trials: ~5% • Canadian adult participation: ~65% • Canadian adult cancer patients: >90% adults treated at “Comprehensive Cancer Centers”
Innovations continued… “I am writing on behalf on my friend's sick child. Could you please send me some information on international treatment resources available for a child who has leukemia, acute lymphoblastic form. This is a boy and he lives in Ukraine. Resources are limited there, but I heard that in Russia some clinics successfully treat this disease. If you need more information about him, please let me know. Please, help us to find a way to help the child.”
Innovations continued… • Increase collaborative international research through international clinical trial participation (Internationally, only 1 in 5 children have access to childhood cancer treatment.)
Access to Information • Utilization of common, comprehensive child-specific clinical trial information service by academia, COG, individual institutions and industry. • Funding of such clinical trial information services (such as HopeLink).
"Life isn't measured by the number of breaths we take, but by the moments that take our breath away."