Download
1 / 49
510 likes | 656 Views
Hepatitis C and HIV/HCV Coinfection. Alan Franciscus Executive Director, Hepatitis C Support Project Editor-in-Chief, HCV Advocate—www.hcvadvocate.org Editor-in-Chief, HBV Advocate –www.hbvadvocate.org Follow us on Twitter and Facebook : hcvadvocate hbvadvocate. Agenda.

E N D
Hepatitis C and HIV/HCV Coinfection Alan Franciscus Executive Director, Hepatitis C Support Project Editor-in-Chief, HCV Advocate—www.hcvadvocate.org Editor-in-Chief, HBV Advocate –www.hbvadvocate.org Follow us on Twitter and Facebook: hcvadvocate hbvadvocate www.hcvadvocate.org
Agenda Overview of hepatitis C Please hold questions until the end of the first session HIV and Hepatitis C – differences and similarities HIV and Hepatitis Coinfection New Advances in hepatitis C care www.hcvadvocate.org
Hepatitis C Overview HCV Statistics HCV Diagnostics HCV transmission & Prevention HCV Symptoms, Disease Progression, Management HCV Treatment www.hcvadvocate.org
Hepatitis C Statistics U.S. Population • 1.6% overall • ~4 million Americans infected • 3.2 million chronically infected • 2.1% Mexican Americans • 3.4% African Americans www.hcvadvocate.org
Hepatitis C Statistics - Montana • Montana • 967, 440 x 1.6% = ~15,500 people with HCV in Montana • 948 case of hepatitis C (chronic and acute) reported in 2008 • Compare to HIV – 895 cases reported since 1985 • Highest rates seen in American Indians and persons age 45-54 (2008) www.hcvadvocate.org
HCV Diagnostics: Antibody tests • HCV Elisa (EIA) • Most common antibody test • A positive antibody test indicates exposure • It does not indicate current hepatitis C infection • Orasure HCV Antibody Test – more later www.hcvadvocate.org
HC V Diagnostics: Viral Load Tests • Viral Load tests • PCR and TMA 5-10 IU/mL • HCV RNA by branched DNA Assay – > 500 IU/mL • Why Is a Viral Load Test Important? • To confirm active infection • Helps to predict treatment response • Indication that treatment is working ** Viral load does not correlate with disease progression** www.hcvadvocate.org
HCV Diagnostics: Genotype Test • Genotypes (1,2,3,4,5,6) • U.S. population • 70% genotype 1 • 30% genotypes 2 & 3 • Why Is a Genotype Test Important? • Helps predict treatment response • Dictates treatment duration of 24 or 48 weeks www.hcvadvocate.org
HCV Diagnostics: Liver Biopsy • Gold Standard for Determining the Health of the Liver • Measure of inflammation • Extent of scarring (if any) • Non-invasive methods – not as accurate www.hcvadvocate.org
Transmission & Prevention www.hcvadvocate.org
Transmission & Prevention • HCV is not spread by breast feeding, sharing eating utensils or drinking glasses, kissing, hugging • Direct blood to blood transmission route www.hcvadvocate.org
Transmission & Prevention: Tips • Injection and Non-Injection Drugs • Do not share needles, cookers, cottons, straws, pipes or any items that might come into contact with blood • Use bleach to clean • People in Stable Long-Term Monogamous Sexual Relationships • CDC – no need to change current sexual practices – but there is a risk www.hcvadvocate.org
Transmission & Prevention: Tips • Safer Sex • For so called “high risk groups” • Multiple sexual partners, people with sexually transmitted diseases, coinfection with HIV or HBV • Any situation where blood is present www.hcvadvocate.org
Transmission & Prevention: Tips • Mother to Child Transmission • Low risk – about 5-6% • Given the low rate of transmission, pregnancy should not be avoided. • Note: pregnant women can not take interferon or ribavirin • Health-Care Settings • Follow standard/universal precautions www.hcvadvocate.org
Transmission & Prevention: Tips • Tattoos & Piercing • Considered a low risk in commercial setting • Make sure disposable needles and separate ink pots are used and that general safety precautions are followed • Considered a higher risk in other settings • Non-commercial settings such as in prison or on the streets www.hcvadvocate.org
HCV Transmission & Prevention: Tips • Household • Cover cuts or sores • Do not share personal hygiene items (toothbrushes, razors, etc.) • Professional Personal Care Settings • Standard precautions • Disposable equipment • Bring own equipment www.hcvadvocate.org
Fatigue – mild to severe Flu-like symptoms (muscle/joint/fever) ‘Brain Fog’ Liver pain Loss of appetite Headaches Gastro problems Chronic Symptoms • and more…… www.hcvadvocate.org
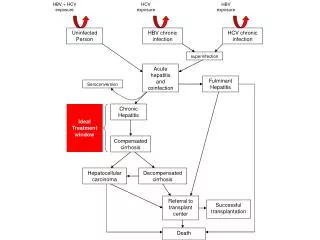
HCV Disease Progression • 10-25% of HCV positive people progress on to serious disease over 10-40 years • Fibrosis • Light scarring • Cirrhosis • Compensated vs. decompensated • Steatosis • Fatty deposits in the liver www.hcvadvocate.org
Disease Progression: Managing Hepatitis C • Regular medical monitoring • Get vaccinated – Hep A & Hep B • Healthy balanced diet www.mypyramid.gov • Exercise • Stress Reduction • Support Groups • Alcohol – Avoid or reduce www.hcvadvocate.org
HCV Treatment • What is interferon? • General antiviral – immune booster • By injection • What is ribavirin? • Antiviral • Used only in combination with interferon • Pill or capsule www.hcvadvocate.org
Merck/Schering – PEG-Intron + Rebetol (800mg) Genotype 1- 41% SVR (48 weeks) Genotypes 2 thru 6 – 75% (48 weeks) Genentech/Roche – Pegasys + Copegus (1000-1200 mg) Genotype 1 – 44-51% SVR (48 weeks) Genotypes 2 & 3 – 82% SVR (24 weeks) Genotypes 2 thru 6 – 70% SVR (48 weeks) *FDA Package Insert Treatment - Standard of Care www.hcvadvocate.org
Interferon Fatigue Muscle/Joint pain Nausea Headaches Anxiety Depression Dry Skin/Rashes And more….. Ribavirin seems to make interferon side effects worse – especially fatigue – Anemia **(both men & women must use birth control) Side-effects www.hcvadvocate.org
Inject before bedtime Drink lots of water Low doses of ibuprofen or acetaminophen Pain medications Small frequent meals Light exercise Daily moisturizing Vary injection sites Anti-Depressants Plenty of rest Managing Side-Effects Key: support from medical providers, family, friends, work – all areas of life www.hcvadvocate.org
Complementary Medicine • Herbs – milk thistle, licorice root, etc. • Always check with your doctor and herbalist – some herbs are unsafe • Acupuncture / Acupressure • Traditional Chinese Medicine www.hcvadvocate.org
Comparisons HIV HCV • Single stranded RNA • Retrovirus • Integrates into DNA • Single stranded RNA • Flavivirus • Does not integrate into DNA www.hcvadvocate.org
Comparisons HIV HCV • Mainly infects CD 4 cells • Daily – replicates billions • High mutation rate • Mainly infects liver cells • Daily – replicates trillions • Very high mutation rate www.hcvadvocate.org
Comparisons HIV HCV • Chronic – 100% • US – 1 major strain • High sexual transmission rate • High IDU transmission rates (Blood) • Chronic rates - 55-85% • US – 3 major strains • Low Sexual transmission rate • Very high IDU transmission rates (Blood) www.hcvadvocate.org
Comparisons – Con’t HIV HCV • Cure? • No • Treatment - lifelong • Can become resistant • Cure? • Virological Cure • Treatment 24 to 48 weeks • No resistant issues yet • New direct antivirals will lead to resistance www.hcvadvocate.org
Comparisons – Prevalence HIV HCV U.S. – • ~1,000,000 • U.S. – • ~4,000,000 www.hcvadvocate.org
Guidelines for Prevention of Opportunistic Infections • HIV – Infected persons should be screened for HCV • Patients should be advised on alcohol use • Patients should be screened for HAV & HBV if negative, they should be vaccinated • Patients should be evaluated for liver disease and possible need for treatment • Liver enzymes should be monitored after initiation of HAART *U.S. Public Health Service and the Infectious Disease Society of America www.hcvadvocate.org
Hepatitis C vs. HIV/HCV Coinfection Transmission / Prevention Diagnosing HCV HCV Disease Progression HCV Treatment Response www.hcvadvocate.org
HCV Transmission HCV HIV/HCV Coinfection • Sexual transmission is low (0-3%) • Mother-to-Child Transmission ~5-6% • HCV meds can cause birth defects • Sexual transmission is higher ~ 15-25% • Mother-to-Child Transmission ~25% • HCV meds can cause birth defects www.hcvadvocate.org
Diagnosing HCV Hepatitis C HIV/HCV Coinfection • Antibody Test • HCV Viral load to confirm active infection • Antibody Test • Note: If low cd4 cell count use HCV RNA • HCV RNA to confirm active infection *People with a comprised immune system may not develop HCV antibodies www.hcvadvocate.org
HCV Disease Progression Hepatitis C HIV/HCV Coinfection • Slow rate of disease progression – usually over 10, 20, 30 years • Faster rate of disease progression to cirrhosis – up to 2-3 times faster & can occur in as little as 10 years • HCV coinfection is the leading cause of death among people with HIV www.hcvadvocate.org
Does HCV Make HIV Worse? • Still a controversial issue but most experts do not believe that HCV makes HIV worse • HCV may blunt immune reconstitution www.hcvadvocate.org
Does HIV Make HCV Worse? • HIV accelerates HCV disease progression – doubles the risk for cirrhosis and increases the chance for liver cancer • Some evidence suggests that when HIV is stable – HCV disease progression is slowed in people with HIV/HCV coinfection www.hcvadvocate.org
When and Which to Treat? • Generally, HIV should be under control • Most recommend treat HIV first • HCV – People with HIV/HCV should be considered for HCV treatment • Unless: • CD4 counts less than 200 • Active opportunistic illness www.hcvadvocate.org
HIV Meds and the Liver • Generally, some medications including HIV medications can be difficult for a liver to process • HIV meds temporarily increase liver enzymes and HCV viral load – usually stabilize over time • If ALT’s 4 to 5 times baseline – • Change to more liver friendly HIV medications www.hcvadvocate.org
Recommendations • HIV specialist and liver specialist should closely follow co-infected people • Monitor liver functions especially when on HIV treatment • Switch to more liver friendly HIV medications www.hcvadvocate.org
HCV Treatments • Treatment response rates lower in people with HIV • Genotype 1 up to 29%; Genotype 2,3 up to 62% • Closely monitored for: • Anemia rates up to 50% caused by ribavirin • Thrombocytopenia (low platelets) caused by interferon • Neutropenia (low white blood cells) caused by interferon www.hcvadvocate.org
Ribavirin and HIV Medications • Ribavirin originally developed for HIV, but not effective • HIV medications that should be avoided or used with caution when combined with ribavirin: • D4T (Zerit) • AZT (Retrovir) • DDI (Videx) www.hcvadvocate.org
Psychological Impact • Two or more potentially life-threatening conditions • Lack of awareness • Lack of support www.hcvadvocate.org
Advances in HCV: Diagnostic Tools HCV OraQuick Rapid HCV Antibody Test Venous – whole blood only – clinics $20.00 ? Available some time in 2010 Results in 20 minutes Finger prick and oral swab Filing for marketing approval likely by end of 2010 Approval expected in 2011 www.hcvadvocate.org
Advances in HCV: Diagnostic Tools The Biosensor - handheld Detect infections – HIV, Hepatitis, HINI, STI, Anthrax Tests blood, saliva, urine – the fluid is injected into a small hole in the device Runs on AA batteries - results in 5 seconds Developed by University of New Mexico and Sandia National Laboratories Estimated cost - $5,000 device - $10.00 for chips – 2 years away? www.hcvadvocate.org
Advances in HCV: Treatment IL28B A variation in IL28B called CC genotype = 2-fold increase in response ~80% of those who achieved response (SVR) had CC genotype Partly explained SVR differences in African Americans and Hispanics Test commercially available in August 2010? www.hcvadvocate.org
Advances in HCV : Treatment HCV Protease Inhibitors Telaprevir and boceprevir - genotype 1 - in combination with pegylated interferon and ribavirin Increase efficacy by 10 to 30% Treatment duration - response guided therapy Telaprevir – skin rash – may be whole body rash Boceprevir – higher rates of anemia www.hcvadvocate.org
Advances in HCV: Treatment Medication burden: Telaprevir – every 8 hours Pegylated interferon (sq) once-a-week Ribavirin – taken twice a day Adherence Resistance www.hcvadvocate.org
Advances in HCV: Oral Meds Only Some unanswered questions – are all oral medications viable? Probably a combination of different HCV protease and polymerase inhibitors At least 5 to 10 years away www.hcvadvocate.org
The End Thanks! www.hcvadvocate.org