Download
1 / 21
210 likes | 351 Views
Managed Clinical Networks. Dr C D Baker. Managed Clinical Networks. A new concept first described in the Acute Services Review report in 1998. Managed Clinical Networks. Definition

E N D
Managed Clinical Networks Dr C D Baker
Managed Clinical Networks A new concept first described in the Acute Services Review report in 1998.
Managed Clinical Networks Definition “linked groups of health professionals and organisations from primary, secondary and tertiary care, working in a co-ordinated way, unconstrained by existing professional and Health Board boundaries, to ensure equitable provision of high quality clinically effective services throughout Scotland.” NHS MEL(1999)10. Paragraph 3.
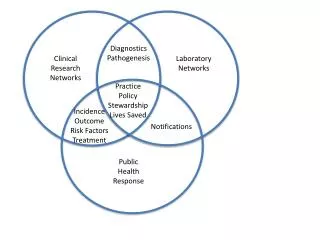
Managed Clinical Networks - core principles. • Managed with structure and clear roles • Purpose is to improve patient care • Evidence based work with use of SIGN and protocols • Outcomes and audit will be an integral part of the work. • A quality assurance programme is required. • Written annual report available to the public. • Networks must be multidisciplinary. • Patients must be involved • HDL(2002) 69
MCNs and policy in NHS Scotland • Concept underpinning Scottish system of NHS co-operation and co-ordination rather than competition and purchasing - important part of health policy. • Policy and strategic planning to be influenced by MCNs • Mandated in some key areas of national priority – CHD, Stroke, Diabetes & Cancer
Managed Clinical Networks - policy documents • Scottish Diabetes Framework • CHD & Stroke Strategy for Scotland • Cancer Plan Scotland • “Our National Health” • “Partnership for Care” • “Future Practice” (report on medical manpower in Scotland)
Local Cardiac MCNs • By April 2004, each NHS Board area should have a local cardiac MCN with a QA programme approved by NHSQIS. • These MCNs will undertake care from initial diagnosis through to chronic management. Rehabilitation and primary prevention is included as well as secondary prevention
Managed Clinical Networks • MCNs have already proved that they can produce benefits for patients. • We wish to see MCNs developed more widely • NHS Boards will be required to support this development
What does an MCN comprise? • All those involved in clinical care and management of disease specific area • Patients and voluntary sector • Manager and support • Lead Clinician
Work of MCN • Clinical work • Support with guidelines, protocols, training etc • Planning and strategy role • Co-ordination and quality assurance • Service development
What can a MCN offer? • Mutual support and sustaining of service • Voice for patients - and influence • Voice for clinicians in planning - locally and nationally • A means of identifying and addressing inequality • Service development and quality improvement
Managed Clinical Networks • Can NHS organisation or structures make any difference to patient care in the real world? • Have we got any evidence about clinical benefit from having a Cardiac MCN in Dumfries & Galloway?
Heart Failure Nursing Service • BHF funding as part of pilot scheme – 100% for 3 years (50% after) • 16 nurses funded – 12 England & Wales, 2 N Ireland, 2 Scotland (D&G) • Application from MCN for nurses to be employed and based in MCN rather than a Trust • Subject to external evaluation (York University) + internal audit (BHF Quality of Life + Athena LVF database based audit)
Heart Failure Nursing Service • To optimise management of patients with established LVF including • Titration & monitoring of diuretics, ACE inhibitors and beta-blockers • Initiation of drug treatment where agreed • Use of non-drug treatments (exercise, O2 etc.) • Referral onwards where appropriate • To provide professional advice and support to patients and carers (+ other health professionals)
HF Nursing evaluation • Formal external evaluation April 02 – December 03 by Dept of Health Sciences, York (Bob Lewin) • 5 (out of 6) centres involved • Bradford • Birmingham • Causeway • Dumfries • Leicester • (major teaching hosp excluded – recruitment problems)
Networks – help survival • Working across boundaries to enable service (and cardiologist) to survive in face of recruitment problems and new GP contract • MIs down by 29% from 2002-3 to 2003-4 – D&G with highest prescribing rate for ACEs, beta-blockers, diuretics, statins etc. in Scotland.
What’s on offer? • A mechanism/ tool/ opportunity to be used or ignored by clinicians and patients • An alternative mechanism to the internal market • A buffer against external private provision of core NHS services/loss of professional autonomy.
Clinical Networks • Individuals make a difference to patient care not structures or protocols • Networks need to support them and make lives easier • Equally it is individuals that make networks succeed and if they are not supported nothing will change