Download
1 / 52
520 likes | 677 Views
The effect of lymph enhancing treatments on tumor development and metastasis . Lisa M. Hodge, Ph.D. Assistant Professor Department of Molecular Biology and Immunology OHF Basic Science Research Chair The National Osteopathic Research Center. The Lymphatic System.

E N D
The effect of lymph enhancing treatments on tumor development and metastasis Lisa M. Hodge, Ph.D. Assistant Professor Department of Molecular Biology and Immunology OHF Basic Science Research Chair The National Osteopathic Research Center
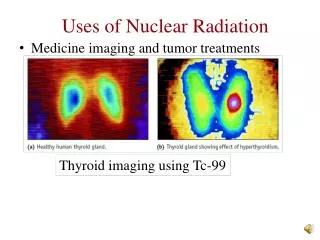
The Lymphatic System • Collects proteins and excess interstitial fluid into afferent lymphatic vessels. • Carries microbial antigens, immune cells, and inflammatory mediators from infected tissues to lymph nodes. • Primed lymphocytes then exit the lymph nodes and enter the lymphatic and blood circulation.
Lymphatic Circulation • Maintained through rhythmic, phasic contraction and external compression of the lymph vessels. • one-way valves along the vessels ensures unidirectional lymph flow . • Respiration, intestinal peristalsis, and muscle contraction facilitate lymph flow. • Exercise, passive limb movement, and body-based manipulative medicine techniques have been shown to increase thoracic duct lymph flow in animals.
Lymphedema • Lymph stasis (lymphedema) may impair immune cell trafficking, leading to infection and tissue/organ damage. • Treatment of lymphedema includes physical therapy, exercise, massage therapy, osteopathic manipulation and compressive garments. • There are few scientific reports on the mechanisms by which these treatments improve lymphedema.
Complementary and Alternative Medicine • Many patients are dissatisfied with conventional medicine and seek alternate treatments • alternative medicine: any healing practice is not conventional medicine • complementary medicine: used in addition to standard care • Many CAM therapies are based on observed historical or cultural beliefs, rather than science • acupuncture, massage, chiropractic medicine, homeopathy, physical therapy, herbal medicine, yoga, diet/exercise, osteopathic medicine • NIH-National Center for Complementary and Alternative Medicine • basic, mechanistic, and/or preclinical research focused on the mechanisms underlying the biomechanical, immunological, endocrinological and/or neurophysiological consequences of manual therapies
Osteopathic Techniques that Enhance Lymphatic Circulation • Myofascial release, traction, and release of diaphragms remove restrictions to lymphatic vessels • Lymphatic pump techniques (LPT) were designed to enhance flow of lymph through the vessels • Thoracic, abdominal, splenic, liver, and pedal pumps • Thoracic pumps are thought to affect the intra-thoracic pressure gradients by augmenting thoracic range of motion and increasing respiratory expiratory efficiency • Abdominal pumps are thought to indirectly affect intra-thoracic and abdominal pressure gradients by intermittently pushing the abdominal contents against the diaphragm.
Clinical applications of LPT • Congestive heart failure • Upper and lower gastrointestinal dysfunction • Respiratory tract infection • Edema • Lymphatic pumps can be applied rhythmically or continuously and typically consist of manual compressions at a rate of 20-30 compressions per minute.
Anecdotal Evidence for the use of Lymphatic Pump Treatments • H1N1 influenza pandemic of 1917-1918, osteopathic physicians reported 110,122 influenza cases, with only 257 cases ending in death. • mortality rate with osteopathic treatment was 0.23% compared to a national mortality rate of 3-5% • mortality rate with osteopathic treatment for patients complicated by pneumonia was 10% compared to the national average of 25% • LPT has also been shown to • increase blood leukocyte numbers • enhance vaccine specific antibodies • enhance bronchial clearance during pulmonary infection • reduce the need for antibiotics during infection • decrease the length of hospital stay in elderly patients with pneumonia • Collectively, these results suggest that LPT can enhance the immune system and protect against infectious disease.
Lymphatic Pump Treatment Increases Thoracic Duct Leukocyte Flux B A • Huff, J.B., Schander, A., Downey, H.F. and Hodge, L.M. Lymphatic Research and Biology 2010; 8(3): 165-69. Hodge, et al. Lymphatic Research and Biology 2010; 8(2): 103-10. Data are means ± SE of the numbers lymphatic leukocytes in dogs (A) or rats (B). * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment Mobilizes Gastrointestinal Lymphocytes into Lymph B A Hodge, et al. Lymphatic Research and Biology 2010; 8(2): 103-10. • Huff, J.B., Schander, A., Downey, H.F. and Hodge, L.M. Lymphatic Research and Biology 2010; 8(3): 165-69. Data are means ± SE of the numbers lymphatic leukocytes in dogs (A) or rats (B). * denotes P <0.05. N=10 animals per group.
Should lymphatic treatments be used in patients with cancer?
Clinical Significance • In the US, approximately one in four women diagnosed with breast cancer will develop secondary arm lymphedema. • tissue injury, surgery, removal of lymph nodes, tumors, radiation therapy • Significant functional limb impairment, psychological morbidity and a reduction of quality of life. • Manual lymph drainage, decongestive lymph therapy and lymphatic/pneumatic pump treatments have been shown to relieve the symptoms of secondary lymphedema. • Many manual medicine therapists are reluctant to perform these lymphatic techniques on patients with cancer • fear of promoting metastasis through the lymphatic system. • Reports suggest the benefits of these treatments in patients with lymphoedema outweigh the risk of adverse events.
Lymph-Enhancing Treatments • Manual lymph drainage, massage and pneumatic/lymphatic pumping • LPT enhances thoracic duct lymph flow in dogs with edema • Both Exercise and LPT increase lymphatic flow and leukocyte numbers • Cancer patients who exercise have a better prognosis • increased killing of tumour cells in vitro • decreased lung metastasis in animal models • increased lymphocyte activation • enhanced survival in animal models • reduced tumour size in rats
Global Hypothesis • LPT will enhance immune surveillance and protection against breast cancer development and metastasis. • Furthermore, we predict that LPT reduce secondary edema due to cancer.
Specific Aims • Specific Aim I: Does LPT protect rats from breast cancer development? • Specific Aim II. Does LPT protect rats from breast cancer metastasis? • Specific Aim III. Does LPT reduce secondary edema in rats with cancer?
Preliminary Data • LPT will reduce pulmonary tumors by enhancing immune surveillance and anti-tumor immune responses within the lungs.
Lymphatic Pump Treatment reduces Solid Tumors and Enhances Leukocyte Trafficking into the Lungs A B Data are means ± SE of the numbers of solid tumors (A) or leukocytes (B) in the lung tissue. * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment Enhances IL-2 Secretion by Pulmonary Lymphocytes Data are means ± SE cytokines (pg/mL). * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment Enhances IL-10 Secretion by Pulmonary Lymphocytes Data are means ± SE cytokines (pg/mL). * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment Enhances IFN-g Secretion by Pulmonary Lymphocytes Data are means ± SE cytokines (pg/mL). * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment Mobilizes Gastrointestinal Lymphocytes into the Lungs of Rats with Pulmonary Tumors • Lung lymphocytes were stained for the gastrointestinal tissue marker a4+b7+. Data are means ± SE a4+b7+ lymphocytes in the lungs. * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment does not Increase Tumour killing in vitro Data are means ± SE the percentage of tumor lysisin vitro. * denotes P <0.05. N=10 animals per group.
Lymphatic Pump Treatment does not Enhance Vascular Endothelial Growth Factor-C Data are means ± SE the serum concentration of vascular endothelial growth factor-C (VEGF-C). N=10 animals per group.
Conclusions • By enhancing the release of GALT derived lymphocytes into lymphatic circulation, LPT enhances immune surveillance and the mucosal redistributionof lymphocytes into the lungs. • In lungs with pulmonary tumors, these lymphocytes secrete cytokines that are important for T cell proliferation, anti-tumor responses and regulation of the inflammatory response. • The killing capacity of these lymphocytes is not enhanced; however, there are greater numbers of NK cells and CD8+ T cells in the lungs of LPT-treated rats. • LPT does not appear to enhance metastasis during the development of solid tumors
Specific Aims • Specific Aim I: Does LPT protect rats from breast cancer development? • Specific Aim II. Does LPT protect rats from breast cancer metastasis? • Specific Aim III. Does LPT reduce secondary edema in rats with cancer?
Rationale • Immunity can suppress tumor development and metastasis. • LPT enhanced anti-tumor immunity and reduced solid tumor formation in the lungs of rats. • The extent to which LPT will reduce solid tumor formation in breast tissue is unknown.
Hypothesis • LPT will enhance anti-tumor immunity and reduce solid tumor formation in the mammary tissue of ratswith breast cancer.
Experimental Design • MTLn3 will be injected into the mammary fat pad of female F344 rats. • Primary tumors will develop within 6 days. • 24 hrs following injection, rats will receive control, sham or LPT treatment for 7 consecutive days. • Primary tumor development will be measured (by palpation, calipers and total body weight) daily. • On day 8 rats will be euthanized, and mammary tissue, lymph nodes, lungs, blood and spleens will be removed for histology, immunostaining, and measurements anti-tumor activities.
Anticipated Results and Limitations • If LPT protect against tumor formation, we anticipate fewer/smaller primary tumors within the breast tissue. • If this protection is immune mediated, we predict more immune cells with anti-tumor activities within the mammary tissue and regional LN. • LPT may enhance immunity but not prevent primary tumor formation • Suggest innate immunity may not be important
Limitations • Enhancing the innate immune response may not protect against tumor development. • Measure the effect of LPT on the adaptive immune response and tumor development • Deplete innate or adaptive immune cell populations and determine if LPT recovers protection against tumor development
Clinical Significance • While the surgical removal of a primary tumor improves the outcome in some patients, it can hasten metastasis in others. • Clinically, if used as a adjunctive therapy, LPT may enhance anti-tumor immunity following the surgical removal of a primary breast tumor.
Specific Aims • Specific Aim I: Does LPT protect rats from breast cancer development? • Specific Aim II. Does LPT protect rats from breast cancer metastasis? • Specific Aim III. Does LPT reduce secondary edema in rats with cancer?
Hypothesis • By enhancing immune surveillance LPT will suppress breast cancer metastasis.
Rationale • Lymph-enhancing treatments have been shown to reduce the symptoms of secondary edema. • There are no published studies documenting that techniques designed to enhance the lymphatic system will promote metastasis.
Experimental Design • MTLn3 will be injected into the mammary fat pad of female F344 rats. • To determine if the application of LPT during primary tumor development will suppress metastasis: • rats will receive control, sham or LPT treatment for days 1-7. • To determine if LPT reduces metastasis following the development of a primary tumor: • control sham or LPT will be applied for days 7-21. • Primary tumor development and lymph node (LN) metastasis will be monitored. • On day 21 rats will be euthanized, and mammary tissue, lymph nodes, lungs, blood and spleens will be removed for histology, immunostaining, and measurements anti-tumor activities.
Anticipated Results • If LPT inhibits breast cancer metastasis during primary tumor formation, we anticipate fewer tumors in the LN and lungs of rats who received LPT on days 1-7 . • If LPT protects during tumor metastasis, we anticipate fewer tumors in the LN and lungs of rats who received LPT during days 7-21. • If protection against metastasis is immune mediated, we also anticipate more immune cells with anti-tumor activities within the mammary tissue, LN, spleens and lungs. • may be localized to sites of metastasis only
Anticipated Results • LPT may not protect against or promote metastasis. • Suggests LPT may safe for the treatment of secondary lymphedema • Conversely, by enhancing lymphatic output, LPT may hasten the lymphatic spread of breast tumors. • identify the mechanism (increased VEGF, enhanced angiogenesis/ lymphangiogensis)
Limitations • The immune response to the primary breast tumor may inhibit tumor metastasis. • Suppression of immunity has been used to enhance metastasis in this model. • Deplete innate or adaptive immune cell populations and determine if LPT protects against metastasis
Clinical Significance • Many clinicians are reluctant to use these therapies in patients with cancer, for fear of metastasis. • There is a need for evidence-based research to identify the potential risks of lymph-enhancing treatments during cancer.
Specific Aims • Specific Aim I: Does LPT protect rats from breast cancer development? • Specific Aim II. Does LPT protect rats from breast cancer metastasis? • Specific Aim III. Does LPT reduce secondary edema in rats with cancer?
Hypothesis • LPT will reduce abdominal edema in rats with intra-peritoneal tumors.
Rationale • LPT has been shown to enhance thoracic duct lymph flow in dogs with edema due to constriction of the inferior vena cava. • The extent to which LPT will reduce edema during cancer is unknown.
Experimental Design • NuTu19 will be injected into the peritoneal cavity of female F344 rats. • Tumors will metastasize to the liver, bowel, ovaries, peritoneum and diaphragm • Abdominal edema will develop within 3-6 weeks • Control, sham or LPT will be applied once there are clinical signs of edema (likely days 21-35). • Abdominal circumference and body weight will me measured daily. • At day 35, rats will be euthanized for necropsy.
Anticipated Results • If LPT is able to reduce abdominal edema, we anticipate reduced abdominal circumference and total body weight. • Alternately, because LPT is applied to the abdomen, it may hasten abdominal metastasis and subsequent edema. • We may find no changes in edema during LPT, suggesting LPT has no effect on edema in this model.
Limitations • NuTu 19 is not a breast cancer, and will be used only as a model for end-stage metastasis and edema. • NuTu19 results in abdominal edema (ascites) • May not correspond to secondary arm lymphedema • NuTu 19 is not immunogenic. • The mechanism by which LPT could potentially reduce edema may be immune-mediated
Clinical Significance • LPT is contraindicated in patients with metastatic cancer, especially if applied to areas where tumors may be present. • The results from these experiments would not only determine if LPT is able to reduce abdominal edema, but would also determine if the application of LPT to areas where tumors are present hastens disease.
Conclusions • By the completion of this research, we will provide scientific support for the use or contraindication of LPT in patients with cancer.Furthermore, we will identify the mechanisms responsible for this outcome. • The results of these studies will help clinicians decide whether or not to use lymph-enhancing therapies, such as LPT, in patients with cancer.
Innovation • We have developed a rodent model that transiently increases lymphatic flow and immune cell release into the lymphatic system • Consistent with our studies in the dog • There are no published reports using animal models to measure the direct effects of enhancing the lymphatic system during cancer.