Download
1 / 42
430 likes | 449 Views
Learn about migraine symptoms, including prodromal signs and aura, and explore emerging therapies for better management. Discover key facts on diagnosis, genetics, and managing chronic daily migraine. Get insights on medication treatments and avoiding analgesic overuse. Find ways to improve lifestyle and prevent relapse for a healthier life.

E N D
Migraine And New Therapies K. Doug Pugar, DO Dayton Center for Neurological Disorders
Migraine is more than just pain… • A non-painful prodromal period can start hours to days before the onset of pain • Fatigue • Mood changes • Yawning • Cognitive symptoms • Excessive thirst • Food cravings • Often the craved foods can be misattributed as “triggers” • Photophobia, phonophobia, osmophobia • Neck stiffness • These symptoms have been shown to be inducible by substances such as nitroglycerin, CGRP, and pituitary adenylate cyclase-activating polypeptide 38 (all known to trigger migraine) • Recognizing the prodromal period can be extremely beneficial; recommend using abortive therapies as soon as these symptoms manifest
Migraine is more than just pain… • Aura • A recurrent and reversible neurologic disturbance • Develops and progresses gradually, lasts minutes • Often sensory, but other CNS symptoms can develop as well • Usually (but not always) followed by a migrainous headache • Headache may also occur simultaneously in some cases • Visual symptoms are most common (“flashing lights,” scintillating scotoma) • And for people with multiple aura symptoms, visual is usually the first • There is often a temporal progression • Others: paresthesias, language difficulties, weakness (focal or generalized) • Treating with abortive medications during the aura may prevent the headache, but usually not the aura itself
Migraine is more than just pain… • Aura – diagnostic criteria
Migraine is more than just pain… • Aura • Genetics • Migraine with aura is more commonly inherited than migraine without aura • FHx of migraine without aura 1.4 – 2 X risk • FHx of migraine with aura nearly 4 X risk • Familial hemiplegic migraine • Aura is severe and prolonged • Pts do not necessarily get more migraines than other migraineurs… the phenotype of the aura is just different
TIA or Migraine Aura? TIA Aura Gradual onset Positive visual and sensory symptoms Flashes / colors Paresthesias • Acute onset • Negative visual and sensory symptoms • Visual field loss • Anesthesia / hypoesthesia
Diagnostic Criteria: Migraine • History of at least 5 headache attacks that last 4-72hrs, with at least 2 of the following features: • Unilateral location • Pulsating quality • Moderate or severe intensity • Aggravated by, or causing avoidance of, physical activity • Headache is accompanied by at least one of the following: • Nausea and/or vomiting • Phonophobia and/or photophobia • May be accompanied by an aura • Spreads gradually • Can involve visual, sensory, speech/language, or motor function
Chronic Daily Migraine • Definition: • 15 or more headache days per month for at least 3 months • At least 8 of these have to be migrainous • Can be unilateral (60%) or bilateral (40%) • Affects about 2% of the adult population • Very disabling and costly • Missed work days • Reduced productivity • ER visits • Only about 20% receive the correct diagnosis
Chronic Daily Migraine • Risk factors: • Analgesic overuse • Obesity • Caffeine overuse • Depression/anxiety/stress • Female sex • Diabetes • Arthritis • Lower education level • Lower socioeconomic status
Chronic Daily Migraine • Pathophysiology • Cortical Hyperexcitability • Increased metabolism (on PET) • Pons • Right temporal cortex • Decreased metabolism • Caudate nuclei • Somatosensory cortices
Migraine Management • Non-pharmacologic management • Routine – regular sleep and eating schedules • Hypersensitive to changes in internal/external stimuli • Biofeedback • Stress management • OMT, massage therapy, chiropractic • Regular exercise • Caffeine cessation • Smoking cessation • Aspartime cessation • Educate about analgesic overuse
Analgesic Overuse • In general, should promote limiting the use of abortive medications to no more then 10 days per month • MORE RECENT DATA • Barbiturate – no more than 5 days • Opioids – no more than 8 days • May lead to glial cell modification • Thus reduced pain tolerance • And reduced response to opioids • Triptans – no more than 10 days • NSAIDS – no more than 10 days • 5 days or less may be protective
Analgesic Overuse • Not all patients who meet criteria for analgesic overuse will have rebound headache • Only way to know is to wean and stop the offending agent • Preventive agents will be less likely to work if a patient is in rebound • For patients that meet criteria, up to 60% will return to episodic migraine once the offending agent is weaned • Often takes several weeks • Education is key! • Watch for relapse
Migraine:Medication Treatments • Only about 22% of migraineurs actually use migraine-specific medications • About 22% use opiates or barbiturates for attacks • Inadequate acute treatment exerts a significant socioeconomic burden and can also promote a transition from episodic to chronic daily migraine
Treatment • Abortive therapies • Triptans • Efficacy rate of 42-76% (depending on the study) • Contraindications • H/o stroke • Hemiplegic migraine • Uncontrolled HTN • Coronary artery disease • Peripheral vascular disease • SSRI/SNRIs? • 2006 FDA report noted a risk for serotonin syndrome when SSRI/SNRIs and triptans were used in combination, but this was based on anecdotal reports • Overall annual incidence in pts using this combo is < 0.03%; this is actually less than the incidence reported for pts on SSRI/SNRI monotherapy • Various modes of delivery available
Triptans • Sumatriptan (Imitrex) – 100mg (PO dose) • Also available as injectable, nasal powder (Onzetra) • Rizatriptan (Maxalt) – 10mg • Eletriptan (Relpax) – 40mg • Zolmitriptan (Zomig) – 5mg • Also available as nasal spray • Almotriptan (Axert) • Frovatriptan (Frova) • Niche for menstrual migraine; take every day during cycle to prevent • Naratriptan (Amerge) • Sumatriptan + naproxen (Treximet) • NOT the same as using the two generics separately; the naproxen is “rapid release”
Triptans • Key points: • Treat early! • If one doesn’t work, try another!
Treatment • Abortive therapies • NSAIDs • Dicolfenac • Cambia – powder • Zipsor – liquid capsule • Naproxen • Ketorolac • Toradol – IV or IM (oral ineffective) • Sprix – intranasal
Treatment • Abortive therapies • Isometheptene-acetaminophen-dichloralphenazone (Midrin) • No longer commercially available, but some compounding pharmacies can provide similar products • Safe with cardiovascular risk factors • Butalbital-acetaminophen-caffeine (Fioricet) • Controlled substance, potentially addictive • Better for tension HA; for migraine, probably no better than placebo • Antiemetics • Promethazine • Prochlorperazine • Metoclopramide • Ondansetron (good for treating migraine-associated nausea, but not particularly for migraine itself)
Treatment • Abortive therapies • DHE • Migranol – intranasal • Avoid long-term use, and avoid if cardiovascular risk factors (arterial constrictors) • Valproic acid • Only helpful abortively if given IV (Depacon), and it must be administered via rapid infusion • 500mg infused over 10 minutes • Oral valproic acid may be helpful as a preventive, but has no use for abortive therapy
Treatment • Pregnancy • No well-designed studies to demonstrate safety of acute therapies • First line = acetaminophen • Good second line option = metoclopramide
Treatment • Preventive therapies • Some guidelines recommend offering preventive therapy to patients averaging 4 or more migraine days per month • Roughly 40% of migraine patients would benefit from prophylactic therapy, but less than 15% actually use it • Relatively high discontinuation rate; about 80% within 12 months • Due to inefficacy or side effects
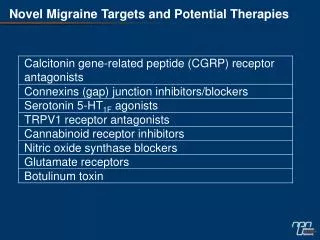
Preventive Therapies • OnabotulinumtoxinA (Botox) • Topiramate (Topamax) • Valproate (Depakote) • Gabapentin (Neurontin) • Amitriptyline (Elavil) • Tizanidine (Zanaflex ) • Others – beta blockers, calcium channel blockers (verapamil), zonisamide, fluoxetine, memantine…
Onabotulinumtoxin A (Botox) • Until recently, was the only FDA approved for treatment of chronic daily migraine • Significant reduction in • Headache frequency • Cumulative hours of headache • Nausea / photosensitivity / phonosensitivity • Disability • Mechanism? • Likely inhibits nociceptor mediators (substance P, glutamate, CGRP) • Reduces peripheral sensitization, and thus central sensitization • Adverse effects : neck pain (9%); head ache (9%); muscle weakness (4%)
Topiramate • Well established as safe and effective • Adverse effects: word finding, fatigue, weight loss, taste, paresthesias, renal stones • Contraindicated in pregnancy! • Recommend 2 forms of birth control for young females • Titrate by 25mg per week • Can be dosed twice daily or as a single nightly dose • New long-acting formulation (Trokendi XR) available • Fewer cognitive side effects • Allows for higher dosing and increase efficacy
Procedural Interventions • Occipital nerve blocks • Supraorbital nerve blocks • Occipital nerve stimulators • Surgical procedures
Complementary and Alternative Therapies • 30-60% may find helpful • Used usually if frequent and intense headaches • Most commonly in addition to Rx therapies • Massage / biofeedback / yoga (most common) • Feverfew (250 mg) • Riboflavin (400 m) • Coenzyme Q 10 (100 mg tid) • Magnesium dicitrate (600 mg) • Butterbur • Daith piercing • Most have no studies with good methodology
Newest Therapies • CGRP Antagonists • Erenumab-aooe (Aimovig) • Fremanezumab-vfrm (Ajovy) • Galcanezumab-gnlm (Emgality) • All with similar efficacy data (no head to head comparisons) • All with excellent side effect profiles • No contraindications • (except “hypersensitivity to drug or any of its excipients”) • Rash, urticaria dyspnea • Fairly easy to get (at least currently) • All have copay assistance programs • Some insurances require a certain number of oral medication failures prior to approval • Some insurances may prefer one over another
CGRPCalcium Gene-Related Peptide • Modulates nociceptive signaling • Activation of the CGRP receptor has been implicated in migraine pathophysiology • Plasma levels of CGRP sampled from the jugular vein have been shown to be higher in migraine patients who are actively experiencing a headache • These levels were shown to return to baseline after triptan administration • In one study, migraine patients were infused with CGRP… All developed a migraine.
Erenumab-aooe (Aimovig) • Approved for both episodic and chronic migraine • Blocks the CGRP receptor • Injected IM monthly • Two dosage strengths approved • 140mg – Half saw a >50% reduction in migraine days • 70mg – 43.3% saw a >50% reduction in migraine days • (26.6% for placebo arm) • Post-hoc analysis • 140mg – 22% saw >75% reduction • 70mg – 20.8% saw >75% reduction • (7.9% for placebo arm)
Erenumab-aooe (Aimovig) • Adverse effects • Injection site reactions most common • Roughly equal in 140 vs 70mg doses, 5-6% • Constipation • 1% of 70mg group, 3% of 140mg group • Muscle cramping • <1% of 70mg group, 2% of 140mg group • Discontinuation rates • 10% for episodic migraine • 5% for chronic migraine
Fremanezumab-vfrm (Ajovy) • Binds to the CGRP ligand • Approved for both episodic and chronic • Dosing: • 225mg IM monthly, OR • 675mg (225 x 3) IM quarterly • Shown to prevent up to 4.6 migraine days per month vs up to 2.5 with placebo, on average (p<0.001) • The monthly dosing was slightly better than the quarterly dosing • Most common side effect: injection site reactions
Galcanezumab-gnlm (Emgality) • 120mg monthly IM injection • Binds to the CGRP ligand • Technically only studied in episodic migraine • But a diagnosis of refractory migraine includes both frequent episodic as well as chronic migraine, so it should be covered in either case • Shown to prevent up to 4.7 migraine days per month vs up to 2.8 with placebo, on average (p<0.001) • Most common side effect: injection site reactions
CGRP-Antagonists • Others to come! • Oral • IV infusion (being investigated for both abortive and preventive therapy)
(937) 478-8751 • Offices in: • Centerville • Beavercreek • Springfield • Eaton • Huber Heights Thank you! Questions? Please call our office to request a referral form
References • Gowers WR. A manual of diseases of the nervous system. Philadelphia, PA: P Blakinston, Son & Co, 1888. • Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia 2018;38(1):1–211. • Afridi SK, Kaube H, Goadsby PJ. Glyceryl trinitrate triggers premonitory symptoms in migraineurs. Pain 2004;110(3):675–680. • Guo S, Vollesen AL, Olesen J, Ashina M. Premonitory and nonheadache symptoms induced by CGRP and PACAP38 in patients with migraine. Pain 2016;157(12):2773–2781 • Headache Classification Committee of the International Headache Society (IHS). Cephalalgia. 2013;33(9):629-808. • Headache Classification Committee of the International Headache Society. The international classification of headache disorders, 3rd edition. Cephalalgia 2018;38(1):1–211. • Hansen JM, Goadsby PJ, Charles AC. Variability of clinical features in attacks of migraine with aura. Cephalalgia 2016;36(3):216–224. • Viana M, Sances G, Linde M, et al. Clinical features of migraine aura: results from a prospective diary-aided study. Cephalalgia 2017;37(10):979–989. • Russell MB, Iselius L, Olesen J. Migraine without aura and migraine with aura are inherited disorders. Cephalalgia 1996;16(5):305–309. • Bigal ME, Borucho S, Serrano D, Lipton RB. The acute treatment of episodic and chronic migraine in the USA. Cephalalgia 2009;29(8):891–897. • Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007;68(5):343–349. • Pringsheim T, Davenport WJ, Marmura MJ, et al. How to apply the AHS evidence assessment of the acute treatment of migraine in adults to your patient with migraine. Headache 2016;56(7):1194–1200. • Cameron C, Kelly S, Hsieh SC, et al. Triptans in the acute treatment of migraine: a systematic review and network meta-analysis. Headache 2015;55(suppl 4):221–235.
References • Becker WJ. Acute migraine treatment in adults. Headache 2015;55(6):778–793. • Evans RW, Tepper SJ, Shapiro RE, et al. The FDA alert on serotonin syndrome with use of triptans combined with selective serotonin reuptake inhibitors or selective serotonin-norepinephrine reuptake inhibitors: American Headache Society position paper. Headache 2010;50(6):1089–1099. • Shapiro RE, Tepper SJ. The serotonin syndrome, triptans, and the potential for drug-drug interactions. Headache 2007;47(2):266–269. • Hansen JM, Thomsen LL, Olesen J, Ashina M. Coexisting typical migraine in familial hemiplegic migraine. Neurology 2010;74(7):594–600. • Hansen JM, Goadsby PJ, Charles A. Reduced efficacy of sumatriptan in migraine with aura vs without aura. Neurology 2015;84(18):1880–1885. • Lipton RB et al. Neurology. 2007;68:343-349 • Hepp Z et al. Cephalalgia. 2017;37(5):470-485 • Emgality [Prescribing Information]. Indianapolis, IN: Lilly USA, LLC. • Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine: A disorder of sensory processing. Physiol Rev. 2017;97:553-622. • Aimovig (erenumab-aooe) prescribing information. 2018. Amgen Inc. Thousand Oaks, CA. • Goadsby PJ, Reuter U, Hallstrom Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377:2123-2132. • Brandes JL, Dolezil D, Freeman MC, et al. Chronic migraine treatment with erenumab: responder rates. Poster presented at 18th Congress of the International Headache Society; Sept 7-10; Vancouver, Canada. • Brossner G, Reuter U, Dodick D, et al. Achievement of > 75% and 100% response in patients treated with erenumab; 24-week results from the STRIVE study. Poster presented at 18th Congress of the International Headache Society; Sept 7-10; Vancouver, Canada.