Download
1 / 20
200 likes | 325 Views
Phylogenetic Insight into HIV Transmission Networks in a Southeastern US Cohort . Ann Dennis 1 , Stéphane Hué 2 , Christopher Hurt 1 , Sonia Napravnik 1 , Deenan Pillay 2 , and Joseph Eron 1 1 University of North Carolina at Chapel Hill; 2 University College London, UK .

E N D
Phylogenetic Insight into HIV Transmission Networks in a Southeastern US Cohort Ann Dennis1, Stéphane Hué2, Christopher Hurt1, Sonia Napravnik1, Deenan Pillay2, and Joseph Eron1 1University of North Carolina at Chapel Hill; 2University College London, UK
New HIV diagnoses continue in the US Southeast • Minorities hardest hit in North Carolina: • Blacks accounted for 66% of new diagnoses in 2009 • Latinos account for 8% ( from 1% in 1995) • Primarily sexual transmission => MSM ~55% of new diagnoses ( from 49% in 2004) North Carolina DHHS. 2010 Epidemiologic Profile for HIV/STD Prevention & Care Planning. www.epi.state.nc.us/epi/hiv/
Phylogenetic inference using HIV-1 pol sequences • Population based sequence data can help characterize the structure of epidemics - a new approach to HIV epidemiology • Paired with epidemiologic data, may provide insight into groups responsible for on-going transmission1 • Pol sequences derived from HIV resistance testing have sufficient variability to allow phylogenetic reconstruction2 1Chalmet K, et al. BMC Infectious Diseases. 2010;10(1):262. 2Hué S, et al. AIDS 2004;18(5):719-728
Objectives Overall Use phylogenetic analyses of HIV pol sequences in conjunction with epidemiologic data to better characterize groups where ongoing HIV transmission is occurring in North Carolina or identify potential gaps in HIV case finding Specific • Determine composition of transmission clusters (n≥3 individuals) • Assess factors associated with cluster membership for newly diagnosed subset (2000-2009)
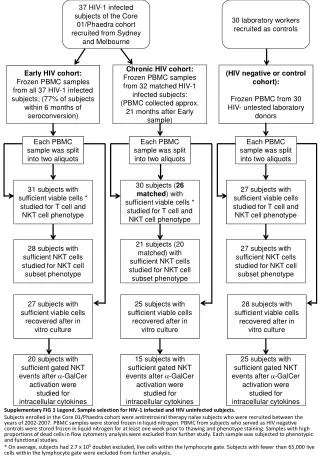
Study Population – 1672 Patients Inclusion Criteria: • one pol sequence available (earliest sequence used) • HIV Subtype B 1. UNC CFAR Clinical Cohort (n=1373) “Unknown”/chronic duration 44% ART naïve; sequences collected 1997-2009
Study Population – 1672 Patients Inclusion Criteria: • one pol sequence available (earliest sequence used) • HIV Subtype B 1. UNC CFAR Clinical Cohort (n=1373) “Unknown”/chronic duration 44% ART naïve; sequences collected 1997-2009 2. Duke-UNC Acute HIV Consortium (n=298) 100% ART-naïve; sequences collected 1998-2009
Sequence sampling was proportional to racial demographics Sequences • Derived from commercial genotypes • Full PR and partial RT (codons 1-400) • Resistance mutations identified Race/Ethnicity: 59% Black , 30% White, 7% Latino
Phylogenetic Analyses • Censored major drug resistance mutations • Selected closely related sequences using Neighbor joining: ≤4.5% pairwise genetic distance (nucleotide substitutions/site) with at least one other sequence • Bayesian trees inferred using GTR+G model of nucleotide substitution
Phylogenetic Analyses • Censored major drug resistance mutations • Selected closely related sequences using Neighbor joining: ≤4.5% pairwise genetic distance (nucleotide substitutions/site) with at least one other sequence • Bayesian trees inferred using GTR+G model of nucleotide substitution • Transmission clusters: • Clades with ≥3 sequences (individuals) • Rigid statistical support confident cluster members share this ancestor
Discrete onward transmission among MSM and heterosexuals Majority: >50% of members share same transmission risk Homogenous: 100% of members share same transmission risk
Clusters are associated with race Majority: >50% of members are same race/ethnicity Homogenous: 100% of members are same race/ethnicity
We found 5 Clusters with majority Transmitted Drug Resistance *all 5 members with same mutation
Multivariable analysis: Factors associated with cluster membership for patients diagnosed 2000-2009 *Referent group Black race Variables not significant: year of diagnosis, sex, transmission risk, ART-naïve status, genotype <1 year of diagnosis, duration of infection (unknown/acute/recent), CD4 count, RNA viral load (closest to diagnosis)
Limitations • Reconstruction of networks only an estimate of the local epidemic • Incomplete sampling – individuals undiagnosed, receiving care at another clinic, or who never had a genotype will be missed • Cannot tell directionality of transmission • Only including clades with very robust statistical support may underestimate number of clusters
Conclusions • Discrete onward transmission among both MSM and heterosexuals • For newly diagnosed patients: non-Latino ethnicity, younger age, and transmitted drug resistance (TDR) were significantly associated with membership in transmission clusters • Younger age and TDR - markers for very high risk behavior and rapid ongoing transmission? • Latino epidemic incompletely delineated
Implications for Intervention • Phylogenetic analyses coupled with traditional epidemiologic data offers additional insight into local HIV epidemics • Identifying groups at highest risk for on-going transmission can lead to enhanced or more targeted intervention programs • Method to evaluate “hidden” populations such as Latino immigrants
Acknowledgments • Co-authors • Patients • UNC Center for AIDS Research • Duke-UNC Acute HIV Consortium • Mike Cohen Supported by: NIAID (T32 AI007001-33), UNC Center for AIDS Research (P30 AI50410), and the Bristol-Meyers Squibb Virology Fellows Research Program