Download
1 / 30
• 310 likes • 530 Views
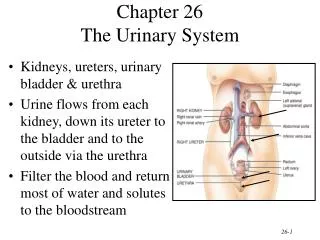
Block: URIN 313 Physiology of THE URINARY SYSTEM Lecture 3. Dr. Amel Eassawi Dr. Shaikh Mujeeb Ahmed. TUBULAR REABSORPTION - 1. OBJECTIVES. Qualitatively describe the forces that determine movement of reabsorbed fluid from interstitium into peritubular capillaries.

E N D
Block: URIN 313Physiology of THE URINARY SYSTEM Lecture 3 • Dr. AmelEassawi • Dr. ShaikhMujeeb Ahmed
OBJECTIVES • Qualitatively describe the forces that determine movement of reabsorbed fluid from interstitium into peritubular capillaries. • Understand pressure natriuresis, pressure diuresis and osmotic diuresis. • State the major characteristics of the proximal-tubular systems for active reabsorption of organic nutrients. • List the approximate percentages of the filtered load of sodium reabsorbed by the various tubular segments. • Understand the active step of sodium reabsorption in all sodium-reabsorbing segments. • Understand the mechanisms of water reabsorption. • Understand the water permeability characteristics of each tubular segment. • Understand the maximum urinary osmolarity. • Define obligatory water loss, and understand its determinants.
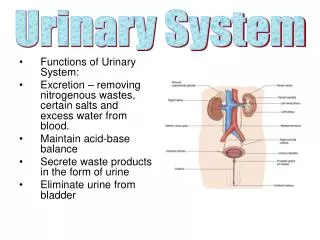
TUBULAR REABSORPTION • All plasma constituents are filtered in the glomeruli except plasma protein. • After filtration, essential material and electrolytes needed are reabsorbed but waste products are eliminated. • Tubular reabsorption is highly selective process. • GFR is 125ml/min, out of this 124ml/min is reabsorbed. 1ml/min excreted. • 99% of water is reabsorbed. • 99.5% Na+ is reabsorbed. • 100% glucose is reabsorbed.
TUBULAR REABSORPTION • There is passive and active reabsorption of different substances. • Passive Reabsorption occurs from tubular lumen to the plasma (trans epithelial transport), when no energy is spent. Movement occurs due to electro-chemical or osmotic gradient. • Active Reabsorption is, when energy is required for trans epithelial transport i.e. when there is movement of substance from tubular lumen to plasma against electro chemical gradient. e.g. Na+ , Glucose, Amino acid, Phosphate (PO4-3)
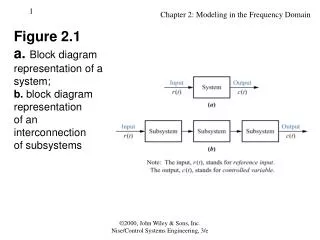
TUBULAR REABSORPTION Trans epithelial transport of substance involves 5 steps: 1. Substance must leave tubular fluid by crossing luminal membrane of tubular cell. 2. Substance must pass through one side of tubular cell to the other. 3. Substance must cross basolateral membrane of tubular cell to enter interstitial fluid. 4. Substance must diffuse through the interstial fluid. 5. It must penetrate the capillary wall to enter blood plasma.
The importance of Sodium Reabsorption • In all nephron segments, the essential event for active transcellular sodium reabsorption is the primary active transport of sodium from cell to interstitial fluid by the Na-K-ATPase pumps in the basolateral membrane. • These pumps keep the intracellular sodium concentration lower than in the surrounding media. The inside of the cell is negatively charged with respect to the lumen, luminal sodium ions enter the cell passively, down their electrochemical gradient.
Sodium Reabsorption Na+ reabsorption is active process i.e. requires Na+ - K+ATPase pump in the basolateral membrane.
Sodium (Na+) REABSORPTION • Na+ is reabsorbed throughout the tubule except descending limb of Loop of Henle, because it is impermeable to Na+ • Na+ Reabsorption in proximal convoluted tubule helps in reabsorption of glucose, amino acid, H2O, Cl-, urea. • Na+ Reabsorption in Loop of Henle occurs with Cl-reabsorption. • Na+ Reabsorption in DCT and CT is under control of hormone Aldosterone. • Principal cells of DCT and CT are the site of action of Aldosterone. • In DCT and CT, 8% of filtered Na+ depends on Aldosterone for reabsorption. If no aldosterone, 20g of NaCl maybe lost per day.
The importance of Sodium Reabsorption • Na+ is filtered and 99.5% of Na+ is reabsorbed in the tubule. • Na+ reabsorption in different areas of tubule. • Proximal convoluted tubule-- 65-67% • Loop of Henle (thick ascending limb) – 25% • Distal and Collecting Tubule – 8%
Role of ReninAngiotensinAldosterone System (RAAS) in various diseases • RAAS activity if abnormally increased can cause hypertension. • RAAS is also responsible for fluid retention and EDEMA occurring in congestive heart failure. • Angiotensin Converting Enzyme inhibitor – ACE inhibitor drugs are used for hypertension and congestive heart failure.
Role of ATERIAL NATRIURETIC PEPTIDE (ANP) in Sodium (Na+) Reabsorption • Hormone ANP causes Na+ loss, therefore, decreases BP. • Natriuretic means inducing Na+ loss in urine. • Site of production of ANP – Atria of heart. • Site of action of ANP – distal part of nephron (DCT and CT), causes decreased Na+ reabsorption, therefore, increased Na+ and water loss in urine. • Inhibits aldosterone secretion from adrenal cortex. • Inhibits renin secretion, therefore, has negative effect on RAAS. • Inhibits vasopressin secretion and its action, therefore causes decreased water reabsorption. • Dilates afferent arteriole and constricts efferent arteriole, therefore, increases GFR. • Relaxes glomerularmesangial cells, therefore, increased Kf – increase GFR
WATER REABSORPTION and EXCRETION • Normal GFR 125ml/min or 180 liters/day • 99 – 99.7% water is reabsorbed • Average urine volume – 1 liter/day • Minimum urine needed per day to get rid of waste products 500ml/day. • Water is reabsorbed through water channels, made up of proteins called Aquaporins. • The water channels in the PCT is Aquaporins AOP-1. The AQP-2 channels in the principal cells of the DCT are regulated by the ADH hormone. • Water is reabsorbed in PCT is 60-70%. It is passive, due to osmotic gradient due to active reabsorption of solutes e.g. Na+
WATER REABSORPTION and EXCRETION • Loop of Henle – 15% of water is reabsorbed. • Descending limb of Loop of Henle [LH] is permeable to water but ascending limb of Loop of Henle is impermeable to water. • Because of this fluid in the descending limb of LH becomes hypertonic and fluid in ascending limb of LH becomes hypotonic. • Distal Convoluted Tubule (DCT) and Collecting Tubule (CT) – 20% of filtered water is reabsorbed. DCT – 5% water reabsorbed. CT – 15% water reabsorbed. • In DCT and CT, water is reabsorbed under the action of ADH (AntiDiuretic Hormone) or Vasopressin. • The principal cells of DCT and CT are the site of action of ADH. • In the absence of ADH most of the water is reabsorped in the PCT.
WATER REABSORPTION and EXCRETION • ADH acts on DCT and CT. There are Aquaporin – 2 (protein water channels) in DCT and CT, principal cells. • Aquaporin – intracellular protein are stored in vesicles in the cytoplasm of principal cells. • Vasopressin causes rapid insertion of these vesicles in luminal membrane of principal cells. • This action of vasopressin (ADH) is mediated by binding of ADH to V2 receptors. • V2 receptors are G-protein which activate cAMP – second messenger system. • As ADH causes water reabsorption in collecting tubules, fluid becomes hypertonic and urine passed is concentrated.
WATER REABSORPTION and EXCRETION • If no ADH, collecting tubule epithelium is relatively impermeable to water in absence of ADH, therefore, large amount of dilute urine will be excreted. • Urine flow may increase to 15ml/min or 22liters/day. • Diabetes Insipidusoccurs due to deficiency of ADH • Nephrogenic DI – occurs when V2 receptors in collecting tubule fail to respond to ADH. • Central DI - occurs due to deficiency of ADH • In both cases, person will pass dilute urine up to 22 liters/day
Pressure Natriuresis, Pressure Diuresis, Osmotic Diuresis • The renal-body fluid system for arterial pressure control is a simple one: • When the body contains too much extracellular fluid, the blood volume • and arterial pressure. The rising pressure in turn has a direct effect to • cause the kidneys to excrete the excess extracellular fluid, thus returning • the pressure back toward normal. • An increase in arterial pressure in the human of only a few millimeters of • mercury can double renal output of water, which is called pressure • diuresis, as well as double the output of salt, which is called pressure • natriuresis. • Osmotic Diuresis – high rate of water excretion caused by the filtration • of poorly reabsorbed solutes such as mannitol.
REFERENCES • Human physiology by Lauralee Sherwood, seventh edition • Text book physiology by Guyton &Hall,11th edition • Text book of physiology by Linda .s contanzo, third edition